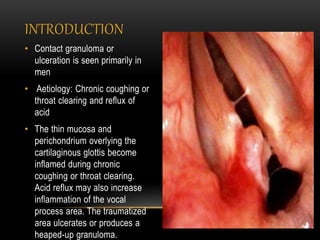
Chronic coughing or throat clearing and acid reflux can cause inflammation and ulceration of the thin mucosa overlying the vocal cords, known as a contact ulcer. A contact ulcer presents as a depressed, ulcerated area with whitish exudate or a bilobed granuloma on the vocal process upon laryngeal examination. Treatment involves modifying voice use to prevent further trauma, antireflux medications, inhaled or intralesional steroids, and microsurgical excision of granulomas as a last resort due to the risk of postoperative recurrence.