Downloaded 51 times
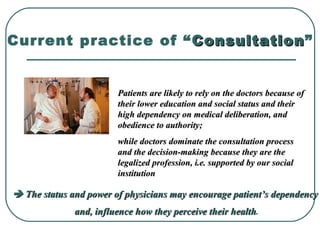
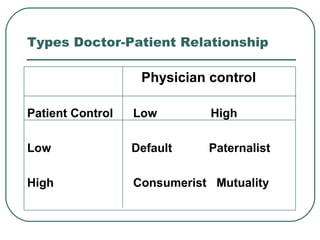


This document discusses the doctor-patient relationship and outlines different types of relationships. It notes that traditionally the relationship has been paternalistic, with the doctor in control and the patient submissive. However, there is a shift toward relationships with shared control and mutuality. The document also examines barriers to effective communication from both the doctor and patient perspectives and provides recommendations for developing a better relationship through openness, active listening, and empowering patients.