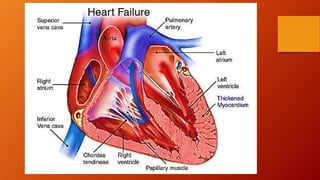
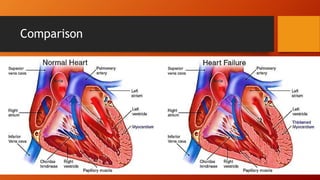
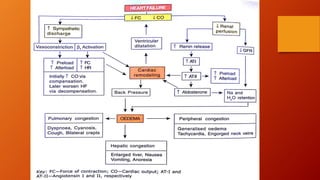
The document discusses heart failure, including common terms, pathophysiology, compensatory mechanisms, and management. It defines heart failure as a condition where the heart cannot pump enough blood to meet the body's needs. Compensatory mechanisms initially help, like increased sympathetic activity and RAAS activation, but over time make the heart work harder and worsen its function. The document compares low vs high output heart failure and left vs right sided heart failure. It describes how compensations eventually fail, leading to decompensated heart failure with symptoms like edema. Management aims to increase cardiac output through drugs that have positive or neutral effects on contractility and preload/afterload.