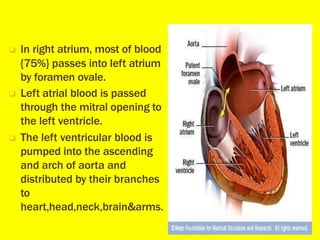
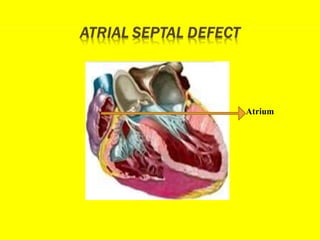
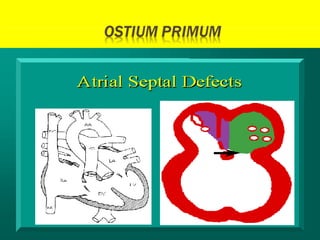
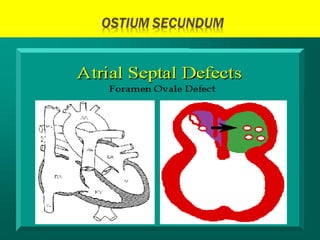
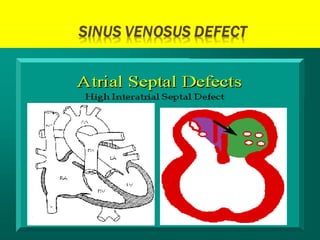
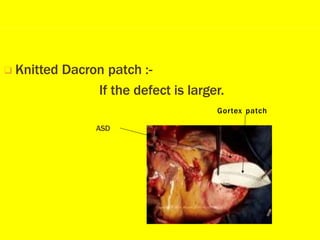
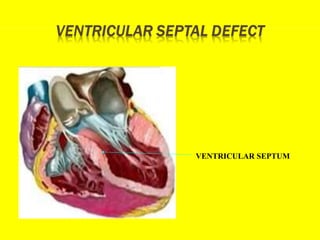
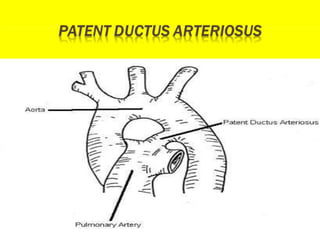
This document discusses acyanotic heart disease, which refers to congenital heart defects present at birth that are not associated with cyanosis. The document defines several types of acyanotic heart defects, including atrial septal defect (ASD), ventricular septal defect (VSD), patent ductus arteriosus (PDA), and coarctation of the aorta. It describes the symptoms, diagnostic testing, potential complications, and treatment options for each condition, which may involve medical management or corrective surgery depending on severity. Early detection and treatment are emphasized to prevent complications as the child ages.