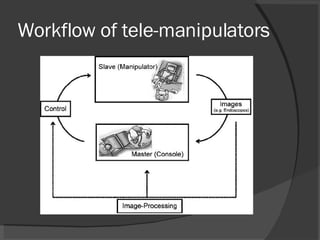
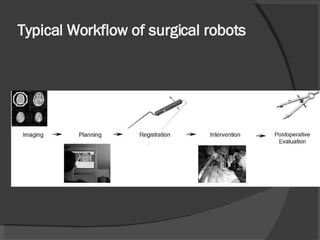
The document discusses computer-assisted interventions in surgery, highlighting two approaches: using robots as tools to assist surgeons or as autonomous systems. It outlines the history of robotic surgery, applications in various medical fields, and details on robotic systems used, such as tele-manipulators and simulators. Additionally, the document addresses case studies related to needle insertion, optimization, control loops, and current trends and challenges faced in integrating robotic systems into surgical practices.