Downloaded 21 times




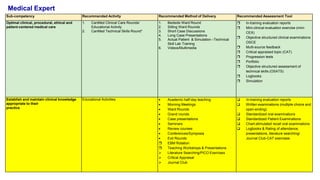
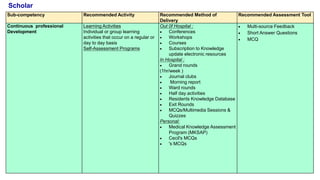
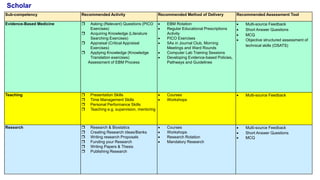
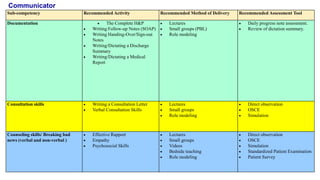
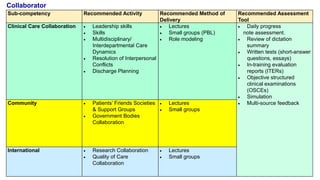
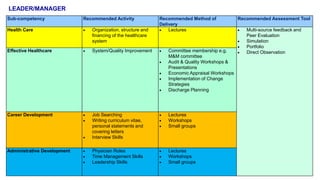
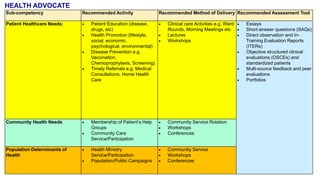
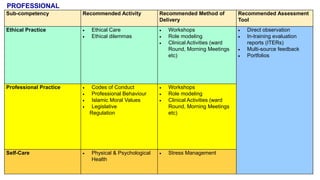
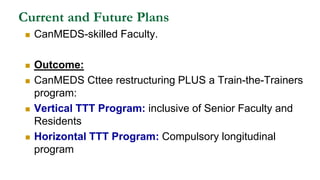
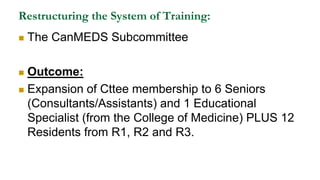

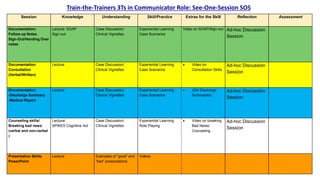
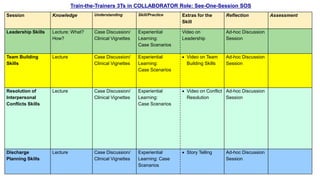
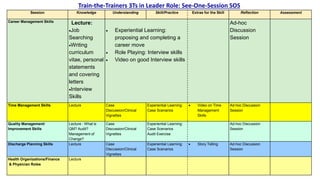



This document outlines plans to restructure medical training at an institution to a competency-based model. It discusses transforming the curriculum, faculty development, assessment tools, and training processes. The plans include establishing competency-focused committees and faculty/resident teams. Training workshops will develop materials for each CanMEDS competency. Assessment tools like online logbooks and end-of-rotation evaluations will evaluate competencies. Educational activities like ward rounds and morning meetings will highlight competencies. The overall goal is to implement a competency-based medical education approach to improve training outcomes.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












