Downloaded 18 times





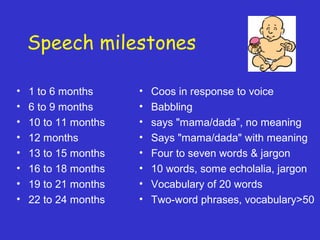
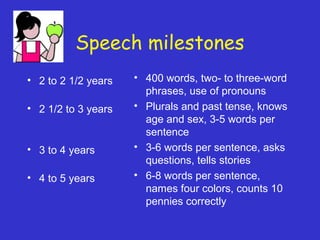


































This document discusses communication disorders in young children. It defines communication and outlines the different forms including nonlinguistic, verbal, and paralinguistic communication. Key communication milestones are provided for different age groups from 1 month to 5 years. Common causes of communication delays like hearing loss, mental retardation, autism, cerebral palsy, and seizures are explained. The document also distinguishes between language disorders and speech disorders and provides an overview of evaluating and diagnosing communication disorders in young children.



































































