This document provides an overview of late talking in young children. It defines key terms related to language and discusses the epidemiology of language delays. Red flags for language delays are outlined for different age groups. Risk factors, potential causes, and the clinical presentation of language delays are reviewed. The natural history, screening recommendations, differential diagnosis, management approaches, and prevention strategies for language delays in young children are summarized.

![Language delay
• No universally accepted definition of "delay“
• children often are considered delayed if their performance on a standardized
assessment of language is at least one standard deviation (SD) below the mean
for age.
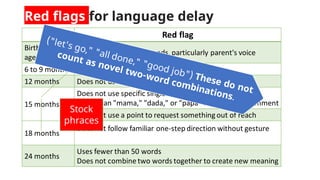
• Red flag generally is the age at which 90%of typically developing children have
attained a clinically predictive skill (eg, 12 months for the use of "mama," "dada,"
or "papa" to call a parent).
Examplesof criteria that may be used
• Scores of 1, 1.5, or even 2 SD below the mean for age.
• Percentage (eg, 25%, 40%) of delay compared with chronologic age. The percentage
delay = (1 - [DA/CA]) x 100 percent,
As an example, an 18-month-old child who has language skills at a 12-month level is 33%
delayed: [1 - (12/18)] x 100 percent.](https://image.slidesharecdn.com/latetalking-220301112112/85/Late-talking-expressive-language-delay-in-pediatrics-5-320.jpg)