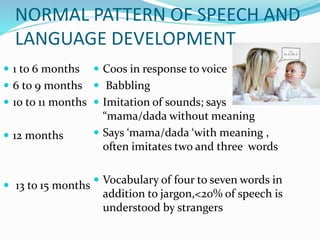
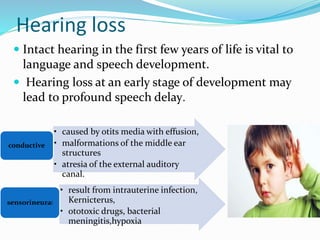
This document summarizes information about speech and language delay in children. It defines speech as the verbal production of language, while language refers to the conceptual processing of communication, including both receptive and expressive abilities. The prevalence of speech and language delay is reported to range from 2.3-19% in children under 5 years old. Causes can include hearing loss, mental retardation, maturation delay, bilingualism, psychosocial deprivation, autism, and various physical factors. The document outlines typical developmental milestones and provides screening tests to evaluate potential delays.