Downloaded 15 times


![A Model for Evidence-
Informed Decision Making
National Collaborating Centre for Methods and Tools. (revised 2012). A
Model for Evidence-Informed Decision-Making in Public Health (Fact
Sheet). [http://www.nccmt.ca/pubs/FactSheet_EIDM_EN_WEB.pdf]](https://image.slidesharecdn.com/healthevidencewebinar-annemartin-apr7-final-160411180739/75/Interventions-with-potential-to-reduce-sedentary-time-in-adults-What-s-the-evidence-12-2048.jpg)
![Stages in the process of Evidence-
Informed Public Health
National Collaborating Centre for Methods and Tools. Evidence-Informed
Public Health. [http://www.nccmt.ca/eiph/index-eng.html]](https://image.slidesharecdn.com/healthevidencewebinar-annemartin-apr7-final-160411180739/75/Interventions-with-potential-to-reduce-sedentary-time-in-adults-What-s-the-evidence-13-2048.jpg)
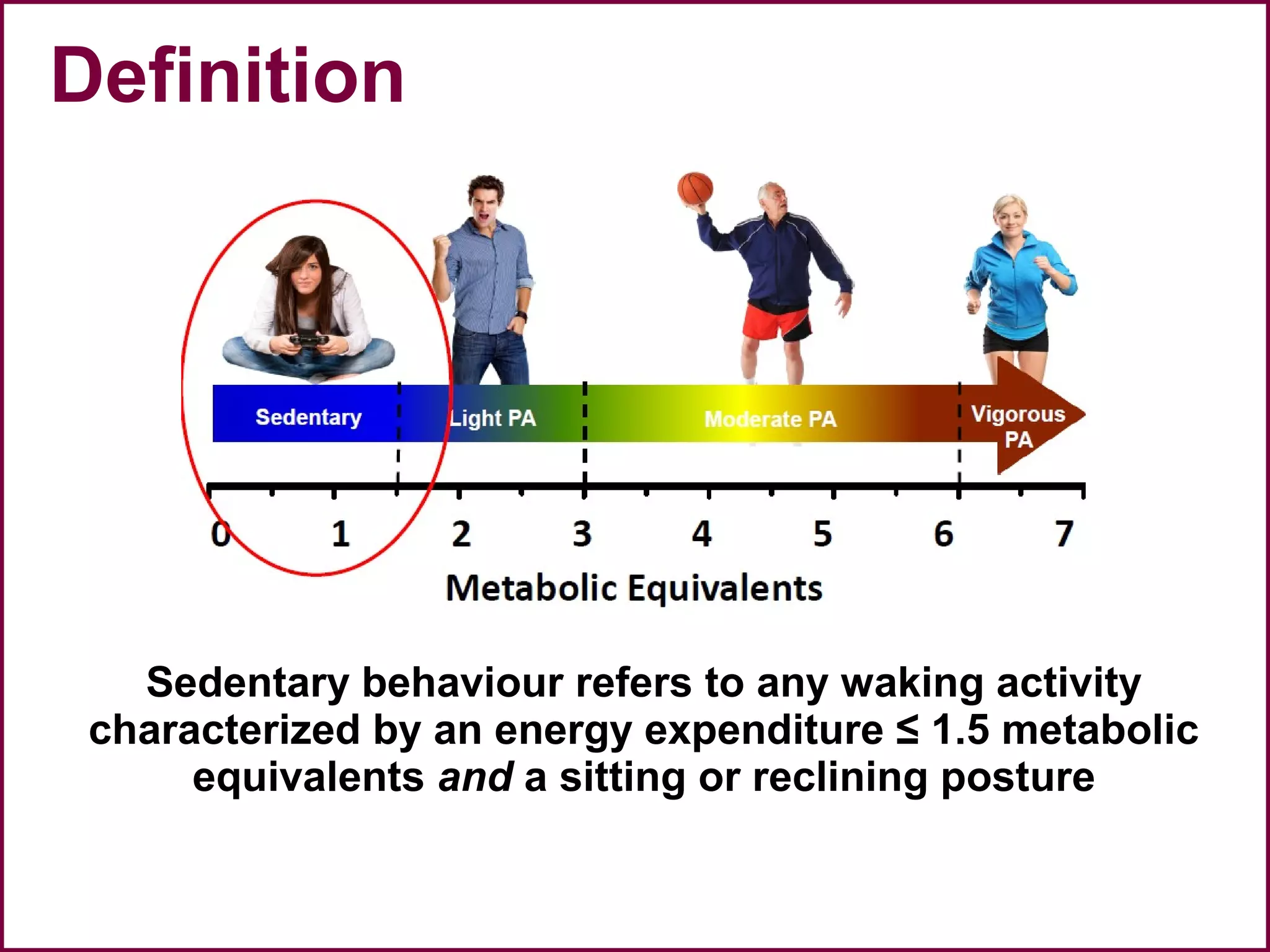
![Sedentary behaviour and
Health
• Significant hazard ratio (HR) associations were found with
– all-cause mortality (HR, 1.220 [95% CI, 1.090 to 1.410])
– cardiovascular disease mortality (HR, 1.150 [CI, 1.107 to
1.195])
– cardiovascular disease incidence (HR, 1.143 [CI, 1.002 to
1.729])
– cancer mortality (HR, 1.130 [CI, 1.053 to 1.213])
– cancer incidence (HR, 1.130 [CI, 1.053 to 1.213])
– type 2 diabetes incidence (HR, 1.910 [CI, 1.642 to 2.222]
• Largely independent of PA but HR bigger with lower PA
Biswas et al. Ann Intern Med. 2015;162:123-132.](https://image.slidesharecdn.com/healthevidencewebinar-annemartin-apr7-final-160411180739/75/Interventions-with-potential-to-reduce-sedentary-time-in-adults-What-s-the-evidence-23-2048.jpg)



![Update search findings
Interventions/
studies
Participants Effect size (min/day)
[95% Confidence
interval]
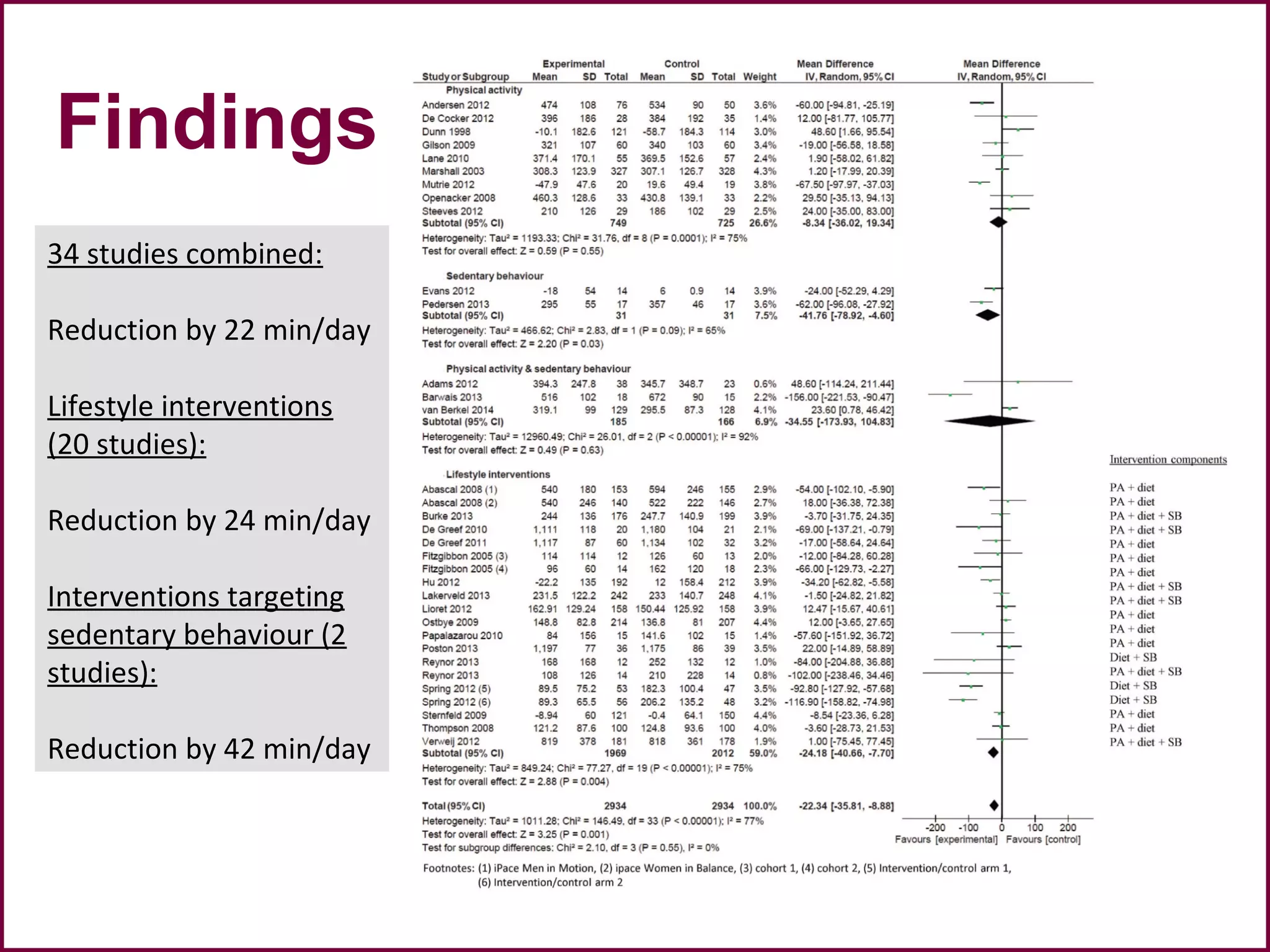
All studies combined 72 20276 -21.54 [-28.20, -14.87]
Physical activity 28 11861 -13.72 [-23.49, -3.95]
Sedentary behaviour 4 264 -45.35 [-75.11, -15.60]
Physical activity & sedentary
behaviour
14 1033 -46.60 [-76.14, -17.05]
Lifestyle interventions 26 7118 -16.74 [-28.16, -5.32]](https://image.slidesharecdn.com/healthevidencewebinar-annemartin-apr7-final-160411180739/75/Interventions-with-potential-to-reduce-sedentary-time-in-adults-What-s-the-evidence-40-2048.jpg)

![A Model for Evidence-
Informed Decision Making
National Collaborating Centre for Methods and Tools. (revised 2012). A
Model for Evidence-Informed Decision-Making in Public Health (Fact
Sheet). [http://www.nccmt.ca/pubs/FactSheet_EIDM_EN_WEB.pdf]](https://image.slidesharecdn.com/healthevidencewebinar-annemartin-apr7-final-160411180739/75/Interventions-with-potential-to-reduce-sedentary-time-in-adults-What-s-the-evidence-46-2048.jpg)

The document provides information about an upcoming webinar on interventions to reduce sedentary time in adults. It includes details about participating in polls during the webinar, obtaining the presentation materials afterwards, and contact information. Participation in the anonymous polling questions is voluntary and intended to stimulate discussion for professional development purposes.