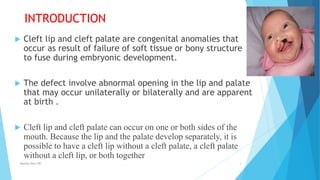
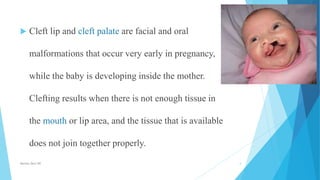
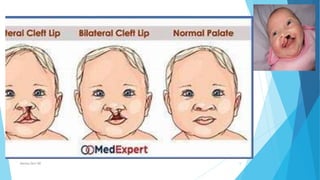
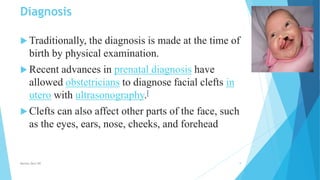
This document discusses cleft lip and cleft palate. It begins by defining cleft lip and cleft palate as congenital anomalies that occur from the failure of tissues in the mouth and lip to fuse properly during embryonic development. The document then covers causes such as genetics and environmental factors. It discusses the pathophysiology of cleft lip and cleft palate in more detail. The rest of the document outlines complications, diagnosis, interventions including feeding techniques and surgical procedures, post-operative care, and monitoring for infection.































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




