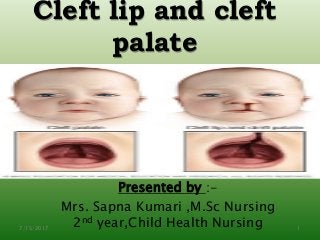

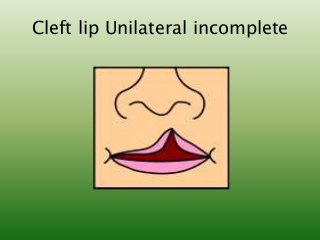
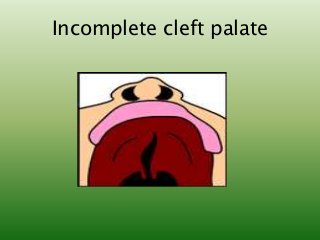
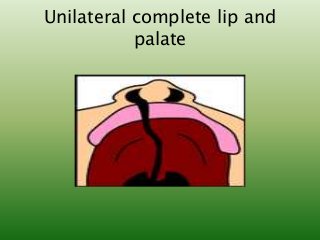
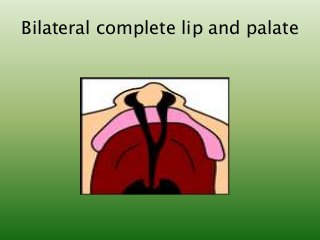






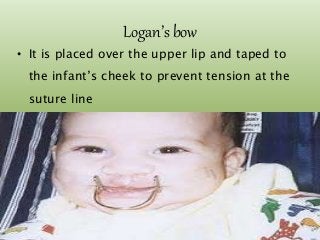




The document provides an overview of cleft lip and cleft palate, defining these congenital malformations and outlining their types, causes, clinical manifestations, and management strategies. It elaborates on the surgical techniques for repair and nursing care involved before and after surgery, as well as potential complications associated with these conditions. Additionally, it includes diagnostic evaluation methods and emphasizes the importance of parental counseling and understanding.

















































































