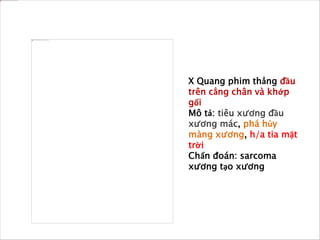
Bệnh nhân 14 tuổi được chẩn đoán có khối u xương ác tính osteosarcoma tại khớp gối phải, cần tiến hành sinh thiết và chẩn đoán hình ảnh để xác định mức độ bệnh. Osteosarcoma là loại u xương nguyên phát phổ biến, thường gặp ở thanh thiếu niên với tỷ lệ xuất hiện cao tại các vị trí xương tăng trưởng. Điều trị bao gồm phẫu thuật kết hợp hóa chất trước và sau phẫu thuật nhằm tăng tỷ lệ sống cho bệnh nhân.














































![[123doc.vn] lam sang noi khoa](https://cdn.slidesharecdn.com/ss_thumbnails/123doc-161209162055-thumbnail.jpg?width=640&height=640&fit=bounds)










































