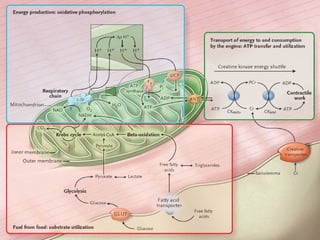
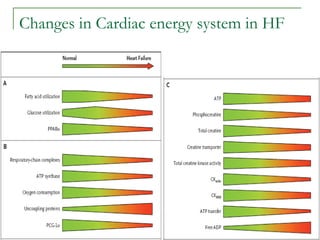
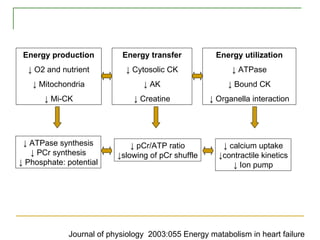
This document discusses cardiac energy metabolism and its derangement in heart failure. It describes how in heart failure there is a shift from fatty acid oxidation to glucose utilization, reductions in oxidative phosphorylation and creatine phosphate levels, and impairments in ATP transfer and utilization. Various molecular regulators of energy metabolism are also discussed, as well as potential strategies for modulating substrate utilization and oxidative phosphorylation as new therapeutic approaches for heart failure.