Downloaded 13 times


![New drug therapies in heart failure-
Nesiritide [synthetic BNP analogue]
Angiotensin receptor neprilysin inhibitor(ARNI)
Levosimendan, pimobendan [myofibril calcium sensitizers]
Recent advances- CCF 20/08/19](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-9-320.jpg)
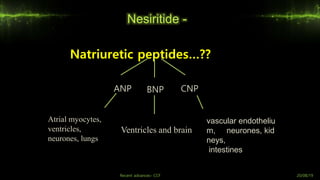
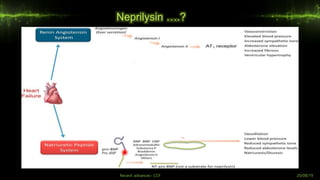
![- Normally, ANP and BNP are expressed in the atria and released on increased preload (stretch).
- During heart failure, ANP and BNP are also produced by the ventricles, such that plasma level
are elevated. [BNP is used as a biomarker of heart failure]
- ANP and BNP stimulate the plasma membrane guanylyl cyclase
Brain Natriuretic Peptide -
Kidney – increased cGMP has diuretic effects
Vessels – increased cGMP has vasodilatory effects
- Heart – increased cGMP has antihypertrophic, antifibrotic effects
Recent advances- CCF 20/08/19](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-13-320.jpg)
![New drug therapies in heart failure-
Nesiritide [synthetic BNP analogue]
Angiotensin receptor neprilysin inhibitor(ARNI)
Levosimendan, pimobendan [myofibril calcium sensitizers]
Recent advances- CCF 20/08/19](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-15-320.jpg)
![New drug therapies in heart failure-
Nesiritide [synthetic BNP analogue]
Angiotensin receptor neprilysin inhibitor(ARNI)
Levosimendan, pimobendan [myofibril calcium sensitizers]
Recent advances- CCF 20/08/19](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-20-320.jpg)
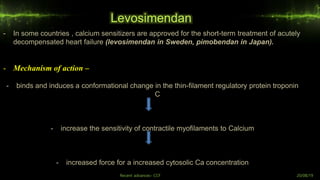
![Levosimendan
- Other actions –
- 1] inhibiting PDE3
- 2] It also opens ATP-sensitive K' channels in vascular smooth muscle cells to cause vasodilatation
- Infused i.v. primarily indicated for short-term treatment of acutely decompensated severe chronic
heart failure
- Though it relieved symptoms of heart failure, but survival rate was not improved.
- Side effects
- The most common side effect is hypotension which may last for few days due to its active
metabolite that has long t1⁄2
Recent advances- CCF 20/08/19](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-24-320.jpg)
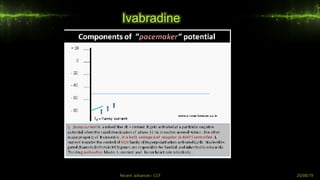
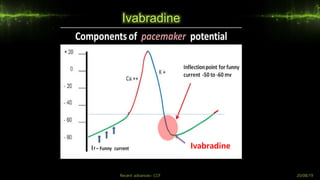
![What so funny about the funny currents..?
Funny currents [If]
Recent advances- CCF 20/08/19](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-26-320.jpg)
![References -
1] O’Connor CM, et al. Effect of nesiritide in patients with acute decompensated heart failure. N Engl J Med, 2011, 365:32
2]Lakatta EG, DiFrancesco D. What keeps us ticking: a funny current, a calcium clock, or both? J Mol Cell Cardiol, 2009,
47:157–170
3] Schober T, et al. Myofilament Ca sensitization increases cytosolic Ca binding affinity, alters intracellular Ca
homeostasis, and causes pause- dependent Ca-triggered arrhythmia. Circ Res, 2012, 111:170–179.
4] Teerlink JR, et al. Serelaxin, recombinant human relaxin-2, for treatment of acute heart failure (RELAX-AHF): a
randomised, placebo-controlled trial. Lancet, 2013, 381:29–39
5] McMurray JJ, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med, 2014, 371:993–10](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-31-320.jpg)
![References -
6]Mebazaa A, et al. Levosimendan for patients with acute decompensated heart failure: the SURVIVE Random
ized Trial. JAMA, 2007, 297:1883–1891
7] Goodman, L., Gilman, A. and Brunton, L. 13th edition, Goodman & Gilman's manual of pharmacology and
therapeutics. Management of heart failure, New York: McGraw-Hill Medical. P1023-47
8] HL Sharma & KK Sharma. Heart failure, sharma and sharma’s principles of pharmacology.3rd edition.
hyderabad, Paras Medical Publisher;2017.p699-847
9] 2017 Focused Update of American Heart Association Guidelines for the Management of Heart Failure](https://image.slidesharecdn.com/recentadvancesccf-191126072818/85/Recent-advances-in-congestive-cardiac-failure-32-320.jpg)



The document discusses recent advances in congestive cardiac failure (CCF), outlining heart failure's definition, classifications, pathophysiology, and treatment options. It highlights the importance of new drug therapies, including nesiritide and sacubitril/valsartan, while addressing the limitations of existing treatments and their associated side effects. Additionally, it emphasizes the need for innovative approaches in managing heart failure due to its high morbidity and mortality rates.








































![Congestive heart fbsbdbbailure [MFKK].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/congestiveheartfailuremfkk-240317144447-689f7db6-thumbnail.jpg?width=640&height=640&fit=bounds)



























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










