1) The document provides guidance for evaluating a patient presenting with chest pain, including conducting a primary survey, focused history, physical exam, and selecting initial diagnostic tests and investigations based on clinical suspicion.
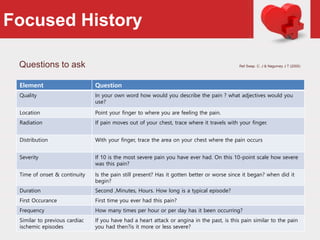
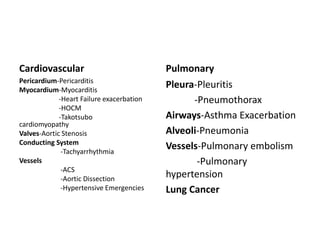
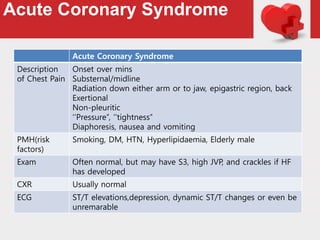
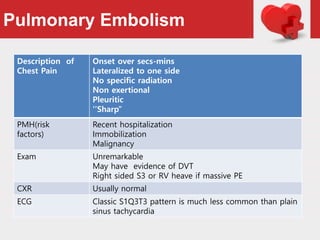
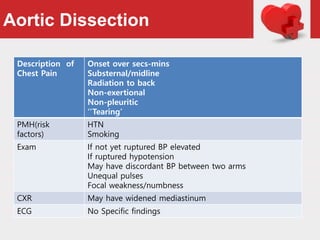
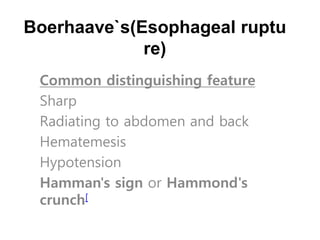
2) Key considerations in differentiating potential deadly causes of chest pain like acute coronary syndrome, pulmonary embolism, aortic dissection, and pneumothorax include analyzing the description of pain, patient history, exam findings, and basic tests like ECG and CXR.
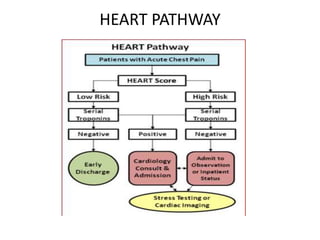
3) While chest pain descriptions and presentations can overlap between conditions, distinguishing features like radiation patterns, exacerbating/relieving factors, exam findings help prioritize the most concerning diagnoses for urgent treatment or further testing. Scoring systems and






















































![Approach to palpitation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/approachtopalpitationautosaved-170805225202-thumbnail.jpg?width=640&height=640&fit=bounds)



























































