Downloaded 25 times
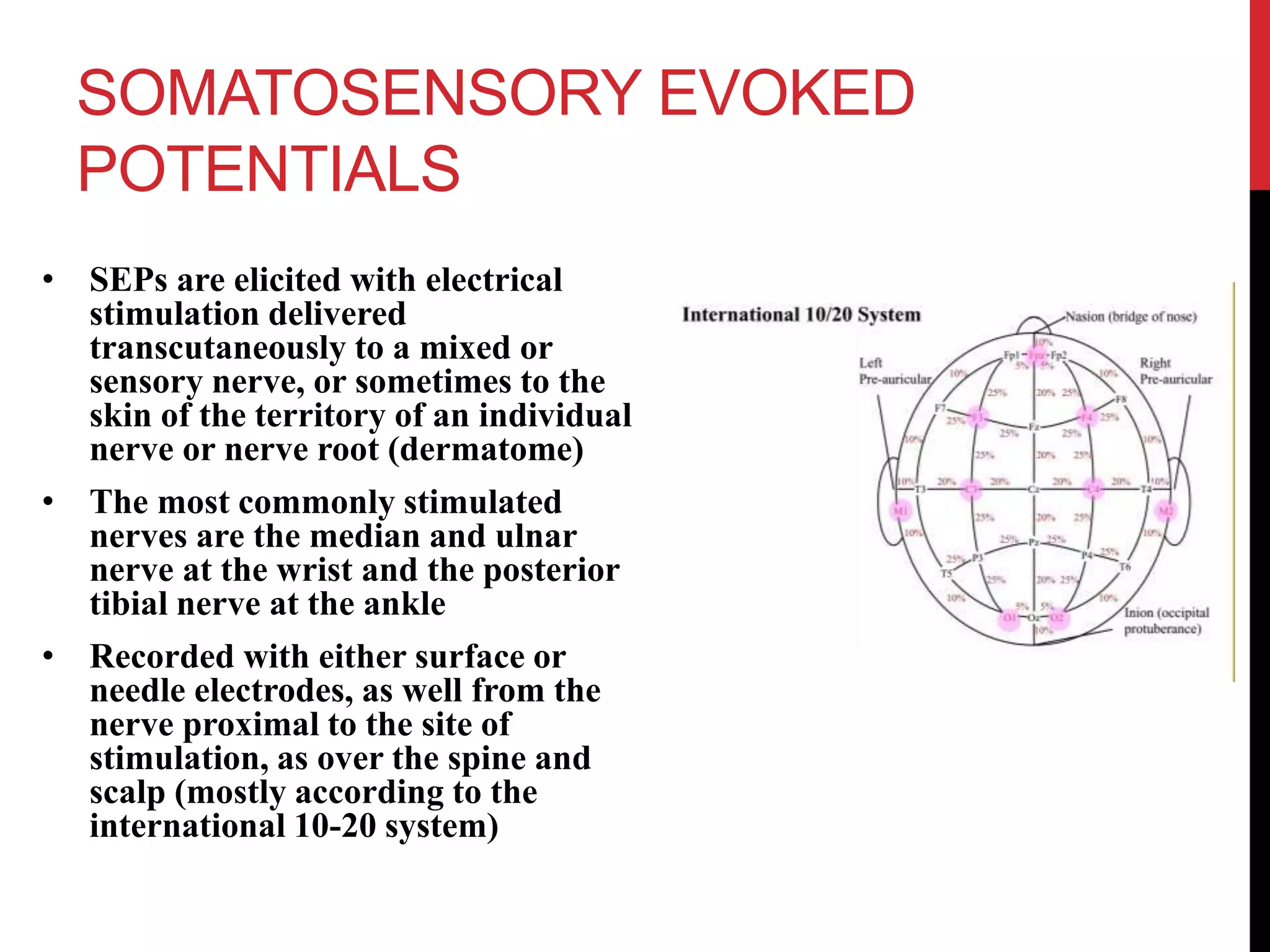


This chapter discusses somatosensory evoked potentials (SEPs) and motor evoked potentials (MEPs) which are used to evaluate spinal cord tracts. SEPs are elicited by electrical stimulation of nerves and recorded from the spine and scalp. They provide information about lesions proximal to the dorsal root ganglion and are useful for diagnosing spinal disorders. MEPs involve transcranial stimulation of motor areas and recording from muscles. They are helpful for evaluating conditions like multiple sclerosis, ALS, spinal cord injury, and stroke. Both SEPs and MEPs have clinical applications in determining prognosis and evaluating treatment for various spinal conditions.




















































































