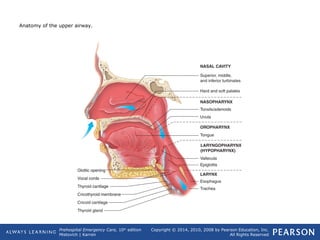
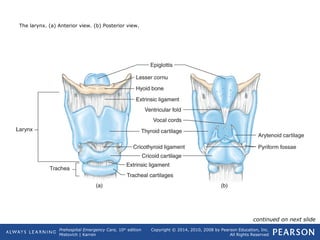
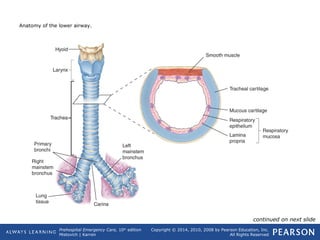
The document discusses respiratory physiology and the pathophysiology of ventilation and respiration. It covers the anatomy and mechanics of the respiratory system, describing the four components of respiration: pulmonary ventilation, external respiration, internal respiration, and cellular respiration. Disruptions to ventilation or respiration can lead to cellular hypoxia, anaerobic metabolism, and organ dysfunction. Impaired pulmonary ventilation can result from interruptions to nervous control, thoracic damage, increased airway resistance, or loss of airway patency.