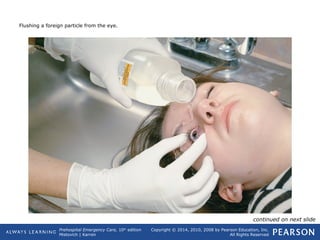
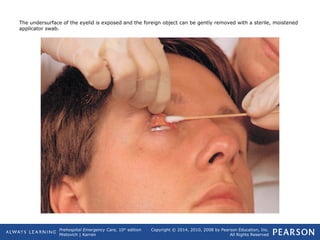
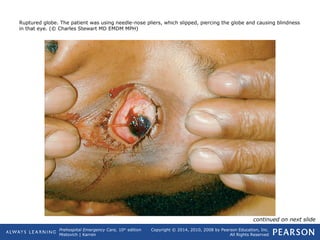
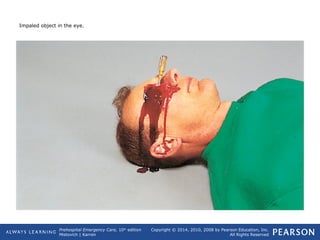
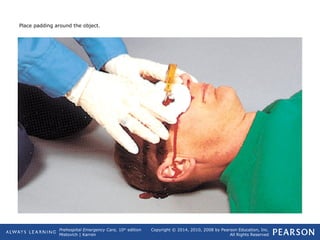
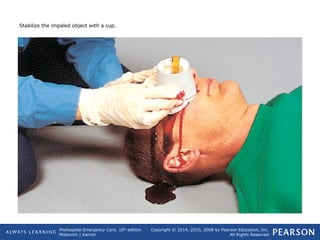
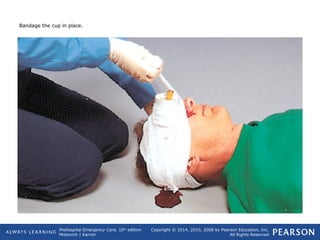
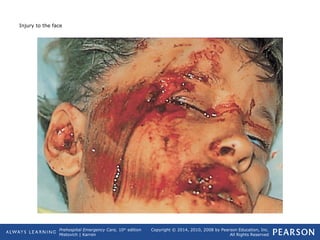
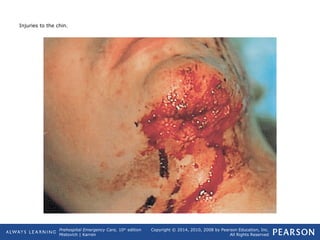
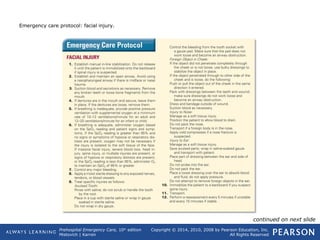
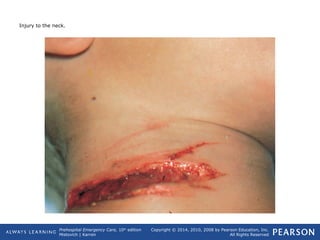
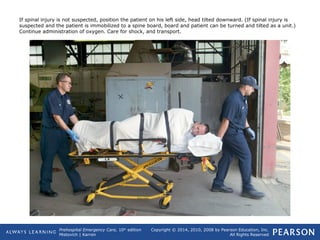
This document provides information on eye, face, and neck trauma from the 10th edition of the Prehospital Emergency Care textbook. It includes sections on anatomy, injuries, and guidelines for assessing and managing various eye, face and neck injuries. Specific priorities for management are establishing an airway, controlling bleeding, and assessing for potential spinal injuries. Injuries require careful examination and monitoring by medical professionals to address issues like foreign objects, lacerations, or potential damage to vision.


















































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




