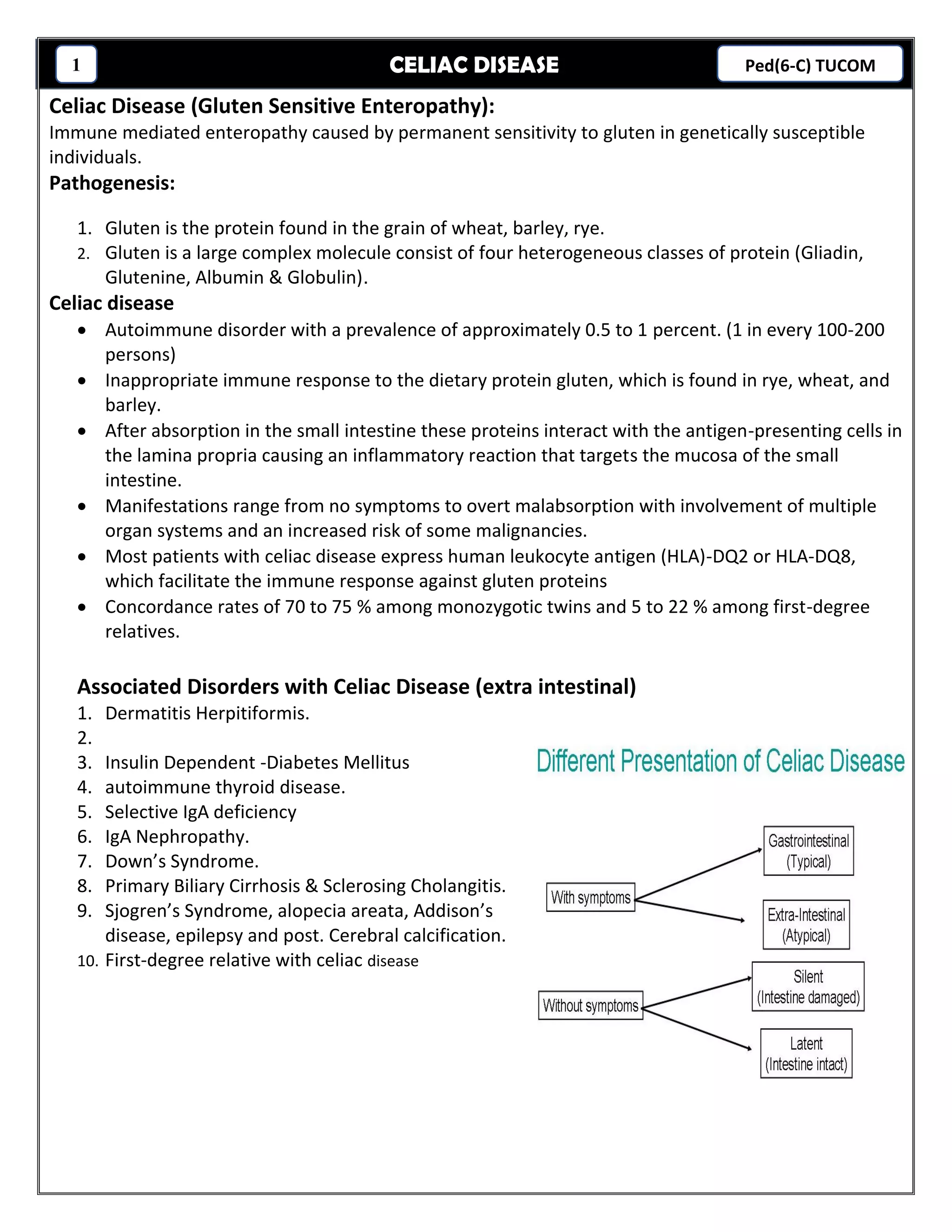
Celiac disease is an immune-mediated enteropathy caused by a permanent sensitivity to gluten in genetically susceptible individuals. It has a prevalence of approximately 0.5-1% and is an autoimmune response to gluten proteins found in wheat, rye, and barley. Diagnosis requires a small bowel biopsy showing villous atrophy and positive serologic markers. Treatment involves a lifelong gluten-free diet to improve symptoms, reverse nutritional deficiencies, and prevent complications like osteoporosis and intestinal lymphoma.