Downloaded 65 times
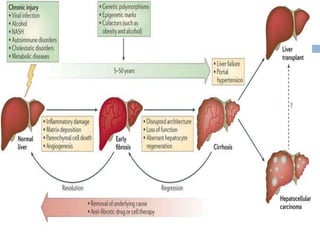
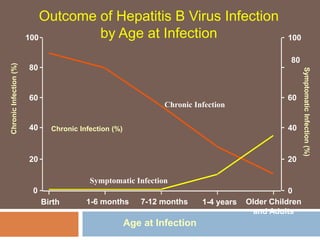
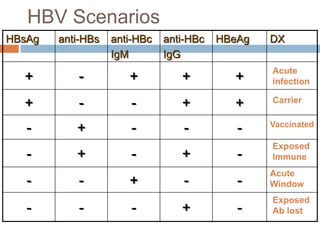
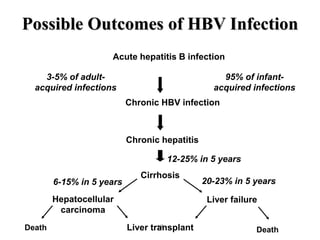
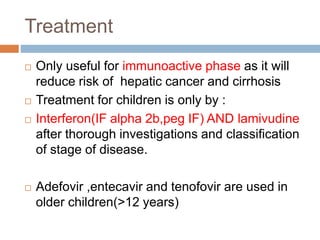
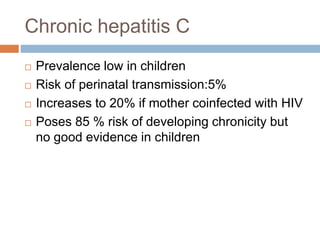
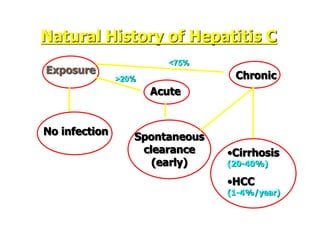

Chronic hepatitis in children can be caused by viral infections like hepatitis B and C, autoimmune disorders, drug reactions, and metabolic diseases. Hepatitis B often becomes chronic if contracted as a newborn. It progresses through immune tolerant, immune active, and inactive carrier phases. Hepatitis C poses a high risk of chronicity in children. Autoimmune hepatitis involves liver inflammation from a misdirected immune response. Common drugs that can cause chronic liver injury include anti-tubercular and anticonvulsant medications. Metabolic diseases such as Wilson's disease and nonalcoholic steatohepatitis account for a significant percentage of chronic liver disease in children. Treatment depends on the underlying cause and may include antiviral therapy,























































































