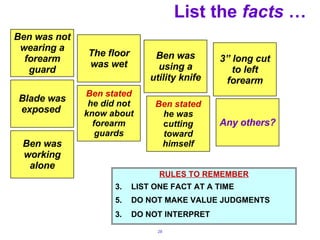
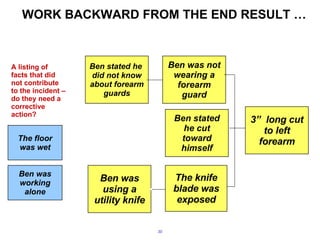
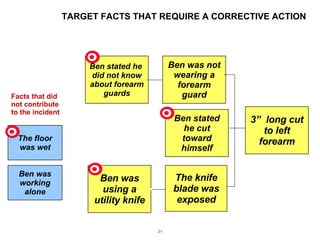
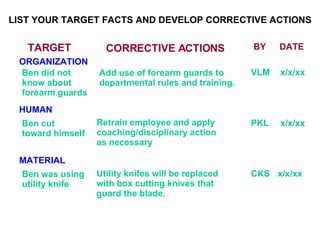
The document discusses root cause analysis training for identifying true root causes of incidents. It explains that root cause analysis involves establishing an investigation team, collecting information, listing facts, and working backwards from the incident result to identify all contributing factors through a "why, why, why" process. True root causes are found by identifying management system failures and addressing both physical conditions and human behaviors. Corrective actions must then be implemented to prevent recurrence.