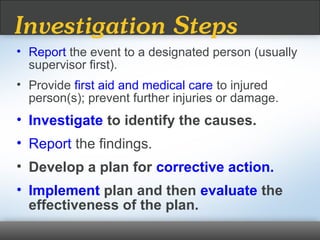
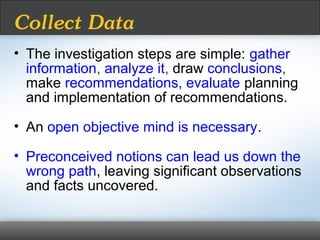
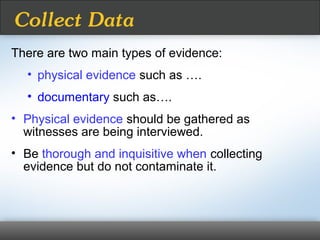
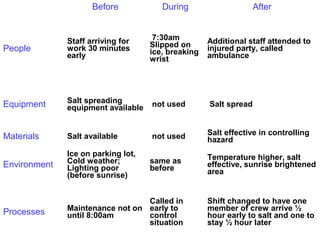
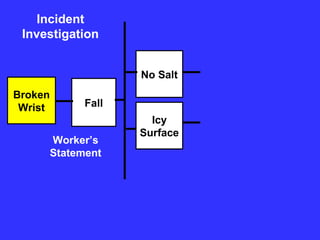
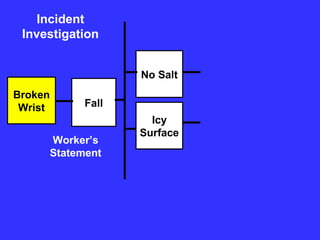
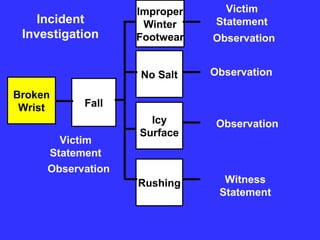
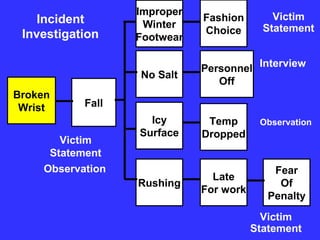
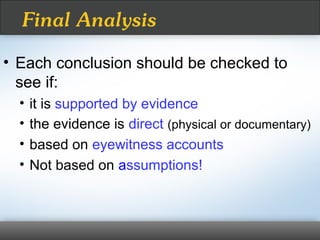
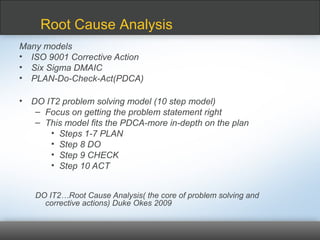
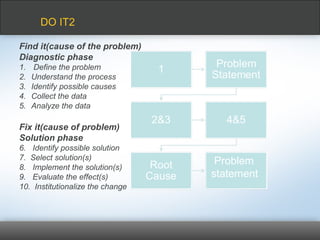
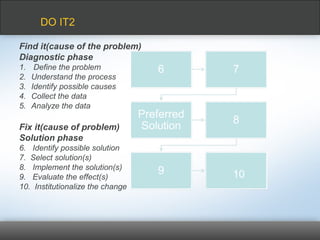
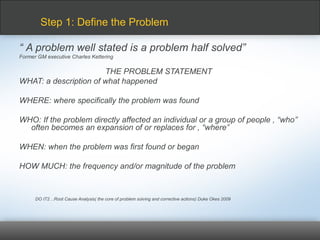
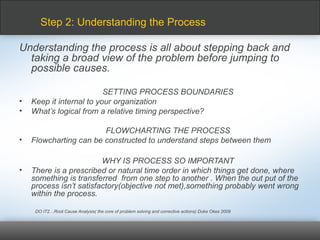
The document outlines the process of incident investigation and root cause analysis, emphasizing the importance of learning from experiences to prevent future incidents. It details steps for gathering evidence, interviewing involved parties, and analyzing data to identify root causes, ultimately leading to corrective actions. Moreover, it highlights the necessity of effective communication, notification requirements under the Nova Scotia OHS Act, and the management of change during the implementation of solutions.



























































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)

![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)





![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)







