BIODATA AND PRESENTING
COMPLAIN
3year old male child weighing 14kg resident of thatta admitted via ER with c/o
• Inability to walk and stand for 14days
• Abnormal movements for 14days
3.
HOPC
• A 3year old boy, with normal growth and
development, came with a 14days history of
inability to walk and continuous involuntary
jerky movements of the body including the
head. His symptoms started 15days before,
following a unprovoked sudden generalized
seizure for about 10mins and then he became
nonambulatory. His mother also noticed a
subsequent progressive mental decline.
4.
• PAST MEDICALHISTORY
Measles at the age of 1 year, remained admitted for 10 days, was on
ventilator support for 3 days
• BIRTH HISTORY
Assisted conception after 5 years of marriage, SVD, Term, Twin
gestation (non identical)
• IMMUNIZATION HISTORY
Unvaccinated
• DEVELOPMENTAL HISTORY
Gross Motor, Fine motor, Social and Speech according to age
• FAMILY HISTORY
5.
• PAST SURGICALHISTORY
• TRANSFUSION HISTORY
• DRUG HISTORY
• PERSONAL HISTORY
• SOCIOECONOMIC HISTORY
6.
EXAMINATION
• On Examination,alert looking child with abnormal asymmetrical continuous jerky
movements of both limbs lying on bed with following vitals:
• HR: 96bpm
• R/R 30breaths/min
• SpO2 at room air: 98%
• Temperature: 98 F
• BP: 96/52 mmHg (on 50th percentile respectively)
• SUBVITALS: A+, J-, CY-, D-, Ed-, Cl-
7.
ANTHROPOMETRIC MEASUREMENTS
• Weight:14 kg (between 25th and 50th
percentile) (SDS -0.44)
• Height: 95 cm (on 50h
percentile) (SDS -0.06)
• OFC: 50 cm (SDS -0.061)
CNS EXAMINATION
• OLFACTORYNERVE: (could not be assessed)
• OPTIC NERVE: (Pupils berl, visual acuity and field of vision could not be assessed)
• OCCULOMOTOR, TROCHLEAR, ABDUCENT NERVE: Intact
• TRIGEMINAL NERVE: Intact
• FACIAL NERVE: Intact
• VETIBULOCOCHLEAR NERVE: (could not be assessed)
• GLOSSOPHARYNGEAL AND VAGUS NERVE: Intact gag reflex
• ACCESSARY NERVE: (could not be assessed)
• HYPOGLOSSAL NERVE: Intact
10.
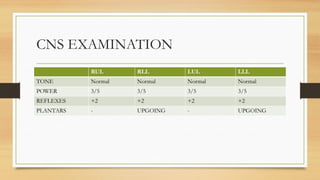
CNS EXAMINATION
RUL RLLLUL LLL
TONE Normal Normal Normal Normal
POWER 3/5 3/5 3/5 3/5
REFLEXES +2 +2 +2 +2
PLANTARS - UPGOING - UPGOING
11.
CNS EXAMINATION
• SENSORYSYSTEM EXAMINATION: INTACT
• CEREBELLAR SIGNS: NO NYSTAGMUS, REST OF THE SIGNS
COULD NOT BE ASSESSED
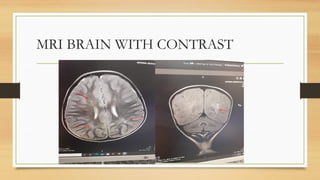
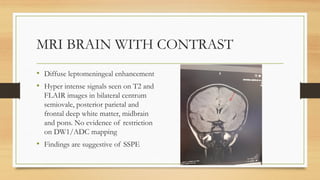
MRI BRAIN WITHCONTRAST
• Diffuse leptomeningeal enhancement
• Hyper intense signals seen on T2 and
FLAIR images in bilateral centrum
semiovale, posterior parietal and
frontal deep white matter, midbrain
and pons. No evidence of restriction
on DW1/ADC mapping
• Findings are suggestive of SSPE
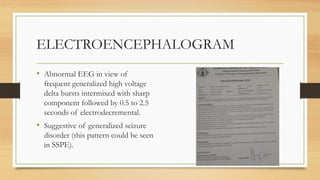
ELECTROENCEPHALOGRAM
• Abnormal EEGin view of
frequent generalized high voltage
delta bursts intermixed with sharp
component followed by 0.5 to 2.5
seconds of electrodecremental.
• Suggestive of generalized seizure
disorder (this pattern could be seen
in SSPE).
19.
CSF FOR OLIGOCLONALBANDS
• Present in CSF indicative of
intrathecal IgG synthesis, No bands
or non matching bands detected in
serum.
20.
CSF FOE MEASLESIgG ANTIBODIES
Patient Antibody Index 2.60- Positive
21.
MANAGEMENT:
• ADMITTED MAINTAINIV LINE
• AT ROOM AIR, NASOGASTRIC TUBE FEEDING
• VITAL MONITORING
• IV ANTIBIOTICS (CEFTRIOXONE 75MG/KG OD)
• IV ANTI EPILEPTICS (LEVITRACETAM 60MG/KG/DAY 8H, CLONAZEPAN 0.01MG/KG/DAY AND SODIUM
VALPROATE 60MG/KG/DAY 8H)
• IV ANTI PYRETICS
• LUMBAR PUNCTURE CONSENT OBTAINED
• MRI BRAIN AND EEG
• KETO DIET AND ISOPRINOSINE
DISCUSSION:
• Subacute SclerosingPanencephalitis (SSPE) is a rare complication due to
persistent measles infection. This neurological sequela typically presents in
early adolescence and has a progressive course with a high mortality rate.
• Vaccination implementation has been effective in reducing the number of
Measles cases, thereby reducing cases of SSPE. However, measles remains
endemic in many countries with poor access to vaccinations. Also, there has
been a re-emergence of measles in industrialized countries due to vaccination
refusal
24.
ETIOLOGY
• Subacute sclerosingpanencephalitis is caused by the measles virus, which is a
single-stranded RNA virus of the Paramyxoviridae family.
• It is one of the most contagious diseases, measles can be transmitted to 12 to
18 persons from one infected individual. Transmission occurs through
aerosols from person to person.
• Many complications can occur both acutely and chronically, some of which
are neurological complications, like SSPE. Children less than five and adults
over the age of 20 are at higher risk of death.
25.
EPIDEMIOLOGY
• Generally, 4to 11 per 100,000 cases of measles result in SSPE. This number goes up to 18
per 100,000 cases if the child was less than five years old when primarily infected with
measles. It appears to have a higher prevalence in males, with later onset and increased latency
in females.
• Risk factors for SSPE include being from a rural area or poverty-stricken area, overcrowding,
multiple siblings, or higher birth order due to an increased chance of exposure and infection
at a younger age (less than 5).
• SSPE tends to have an earlier onset and a more fulminant course in individuals with acquired
immunodeficiency syndrome, children whose mothers had measles during pregnancy, or if
there was an incomplete transfer of measles antibodies during gestation.
26.
PATHOPHYSIOLOGY
• The typicalimmune response to infection starts with T-helper 1 cells that release
interferon-alpha and IL-2. These cytokines help to eliminate the viral infection
from cells. The humoral response then plays a role in making antibodies for long
term protection from the virus. These antibodies will trigger T-helper 2 cells that
release large amounts of IL-4 and a small amount of IL-2 and interferon-alpha.
It is a possibility that SSPE is the result of a poor cellular immune response.
There is evidence to suggest that patients who go on to develop SSPE have a
reduced cellular immune response and an elevated humoral immune response,
which would prevent the patient from completely eradicating the virus.[4]
27.
CLINICAL MANIFESTATION
• Thecourse of SSPE has been divided into stages, each of which describes a certain phase of the
disease.
• Stage I includes many personality or behavioral changes, such as irritability, dementia, lethargy, social
withdrawal, or speech regression.
• Stage II is made up of the progressive decline in motor function, including myoclonus, dyskinesia,
and dystonia.
• Stage III consists of patients who have progressed to extrapyramidal symptoms, posturing, and
spasticity.
• Lastly, stage IV occurs when patients develop akinetic mutism, autonomic failure, or enter a vegetative
state
28.
CLINICAL MANIFESTATIONS
• Atypicalpresentations of SSPE can include psychiatric symptoms, seizure
disorders poorly controlled with medication or solely extrapyramidal
symptoms.
• When atypical symptoms are present, SSPE tends to have a fulminant course
with neurological deficits occurring in the first 3 months or death within 6
months in about two-thirds of cases. Having the measles virus before the age
of 2, increased viral virulence and coinfection with other viruses are risk
factors for a more fulminant, atypical course.
29.
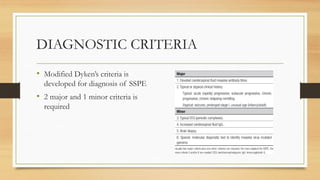
DIAGNOSTIC CRITERIA
• ModifiedDyken’s criteria is
developed for diagnosis of SSPE
• 2 major and 1 minor criteria is
required
30.
TREATMENT
• No cureexists for subacute sclerosing panencephalitis. Most treatments are
aimed at symptom reduction.
• Inosine pranobex is an oral antiviral that halts viral replication and
immunomodulator. The dosing is 100mg/kg/day divided into three doses
throughout the day with a maximal dosage of 3000mg/day. This therapy is
known to cause elevated uric acid in urine and serum samples, as well as
occasional nausea
31.
TREATMENT
• Interferon-alpha (INF-alpha)is another mode of therapy typically used with
Isoprinosine. It is an immunomodulator administered via the intrathecal route
every week. Maximal efficacy of interferon-alpha can only be achieved with
long-term treatments. Some studies have shown that there is no advantage to
daily Isoprinosine plus weekly INF-alpha versus Isoprinosine monotherapy.
• Ribavirin, a nucleotide analog, has also been tried as a supportive treatment.
Little success was noted, and it seemed to only mildly benefit patients when
used in conjunction with INF-alpha.
32.
TREATMENT
• As analternative treatment, several case reports recommend a ketogenic diet.
There has been some variable success with this in reducing myoclonus
symptoms in patients with SSPE who have failed other treatment options.
• This particular diet is neuroprotective in that it reduces oxidative stress,
improves mitochondrial activity, and suppresses factors that induce
apoptosis.
33.
TREATMENT MODALITIES UNDER
STUDY
•Other therapies that are currently being studied in vitro include antiapoptotic
agents and small interfering RNA. siRNA appears to inhibit viral replication
in cells but has not been studied as therapy in humans yet.
• Other studies have recommended the development of therapies that could
block membrane fusion, which could potentially stop the progression of
CNS infections by the measles virus.
34.
PREVENTION
• At thismoment, preventing SSPE from developing is the best treatment option. Vaccination for the measles virus
is a very safe and effective way to prevent initial infection.
• The vaccination is separated into two doses, one given at 12 to 15 months and the second given between the ages
of 3 to 5 years.
• Vaccination cannot be given to anyone who is immunosuppressed because it is a live-attenuated vaccine.
• WHO recommends administering the vaccine to HIV-positive patients in the absence of severe
immunosuppression.
• 95% must demonstrate immunity with anti-measles antibodies to completely eradicate the measles virus from a
population.
• In the last few years, there has been a re-emergence of the measles virus in industrialized countries. This is largely
attributed to reduced vaccination due to vaccine hesitancy
35.
PROGNOSIS
• The mortalityrate is exceptionally high in the case of SSPE, about 95%,
while the remaining cases undergo spontaneous remission. The average life
span after the initial presentation is about 3.8 years, with a range of 45 days
to 12 year.
36.
COMPLICATIONS
• SSPE isa complication of chronic CNS infection by the measles virus. A
patient with SSPE experiences a progressive course of neurological deficits,
which ultimately results in death. Treatments that attempt to prolong and
improve the quality of life can have some side effects/complications.
Interferon-alpha can cause flu-like symptoms or produce a clinical relapse
secondary to antibodies to the interferon. Ribavirin can produce oral
mucositis, headache, fatigue, and reversible anemia.
Editor's Notes
#23 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#24 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#25 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#26 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#27 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#28 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#29 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#30 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#32 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#33 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#34 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#35 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-
#36 Rocke Z, Belyayeva M. Subacute Sclerosing Panencephalitis. [Updated 2023 May 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-



![PATHOPHYSIOLOGY
• The typical immune response to infection starts with T-helper 1 cells that release
interferon-alpha and IL-2. These cytokines help to eliminate the viral infection
from cells. The humoral response then plays a role in making antibodies for long
term protection from the virus. These antibodies will trigger T-helper 2 cells that
release large amounts of IL-4 and a small amount of IL-2 and interferon-alpha.
It is a possibility that SSPE is the result of a poor cellular immune response.
There is evidence to suggest that patients who go on to develop SSPE have a
reduced cellular immune response and an elevated humoral immune response,
which would prevent the patient from completely eradicating the virus.[4]](https://image.slidesharecdn.com/drdanish21aug2025-250830055217-5e134c12/85/Case-presentation-on-subacute-sclerosing-panenecephalitis-pediatrics-26-320.jpg)
























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)