Download to read offline


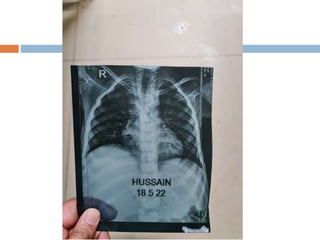
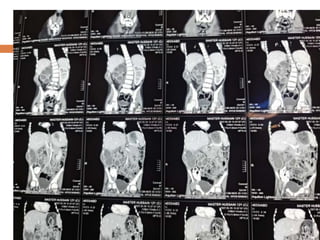
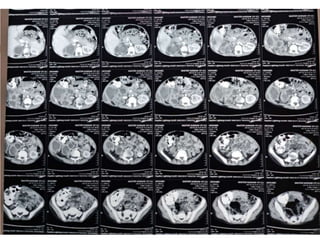
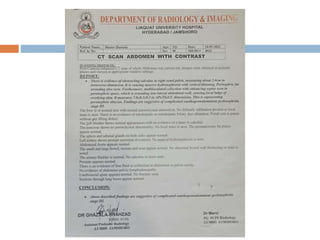
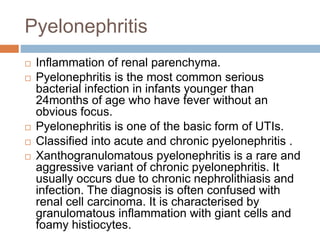
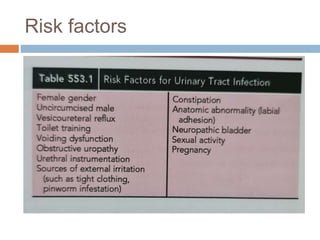



A 12-year-old boy presented with 1 month of fever, right flank pain, and a 15-day history of swelling in the right flank region. His past medical history included a previous hospitalization 2 years prior for fever and right flank pain where he was diagnosed with right renal calculi. On examination, he appeared wasted and pale with tenderness and a hard, mobile swelling in the right flank region. Differential diagnoses included pyelonephritis, renal tuberculosis, and renal cell carcinoma. Pyelonephritis is the most common diagnosis in infants under 24 months presenting with fever without an obvious focus. It is classified into acute or chronic forms, with xanthogranulomatous pyelonephritis




















![[MBBS/MS/DNB] Sample EXAM Long Case on Breast Lump](https://cdn.slidesharecdn.com/ss_thumbnails/cccbreast-200518145117-thumbnail.jpg?width=640&height=640&fit=bounds)





















































