1. This case presents a 40-year-old male with HCM experiencing progressive heart failure symptoms despite medication. Exercise echocardiograms showed provocable outflow obstruction.
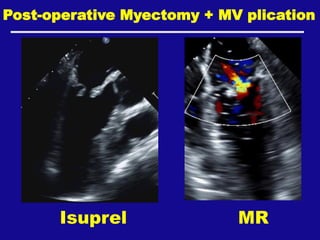
2. The next steps included evaluating and managing his symptoms with disopyramide initially, then myectomy with mitral valve plication which improved his quality of life.
3. For his family screening, his 14-year-old daughter should undergo genetic testing and cardiac screening due to his positive pathogenic MYPC3 mutation.