Downloaded 34 times

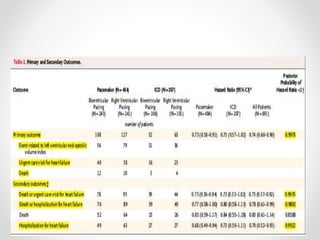
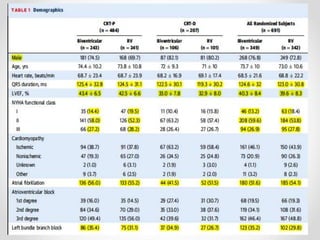

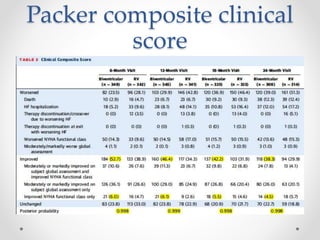
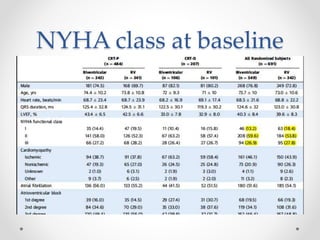
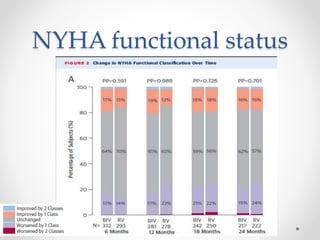
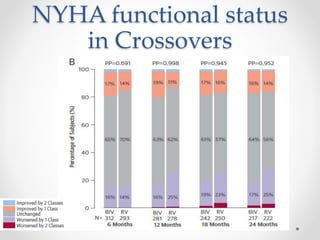
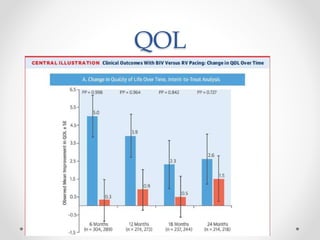
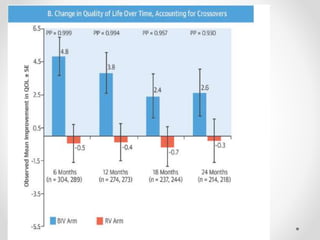


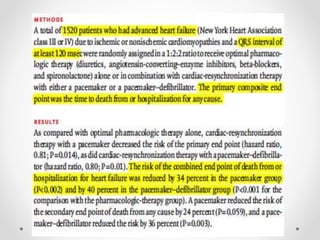
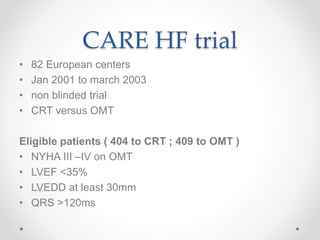
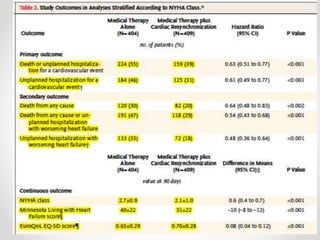
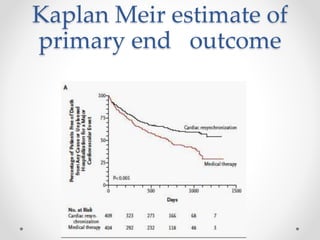
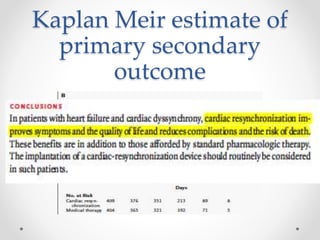
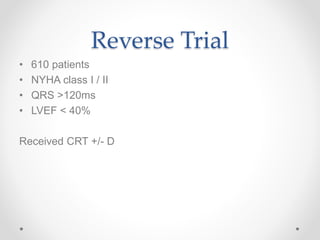
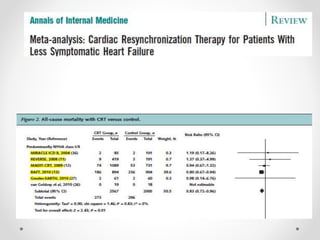
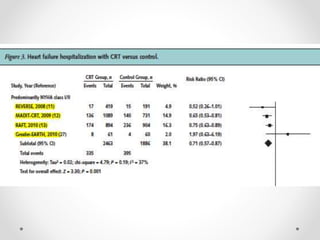
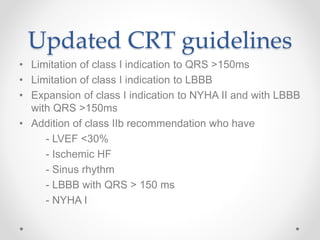
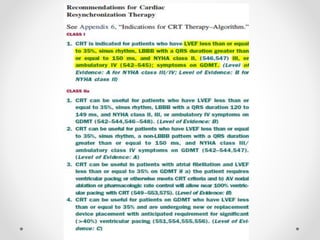
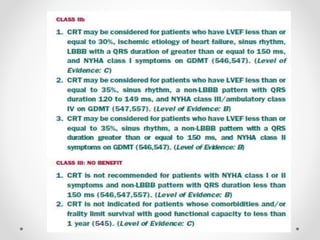

The document summarizes several studies on cardiac resynchronization therapy (CRT) for heart failure. The Block HF trial found that CRT was superior to right ventricular pacing alone in reducing death and heart failure-related events in patients with heart failure, left ventricular dysfunction, and AV block. Subsequent trials like COMPANION, CARE-HF, REVERSE, and MADIT-CRT also demonstrated benefits of CRT over medical therapy alone in improving outcomes like mortality, hospitalizations, quality of life and left ventricular function. Updated guidelines have expanded the use of CRT to patients in NYHA class I/II with left bundle branch block and QRS duration over 150ms.























































































