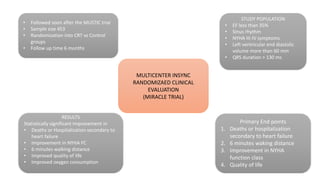
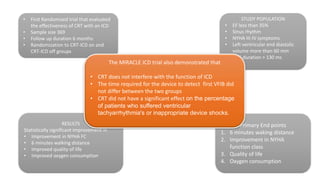
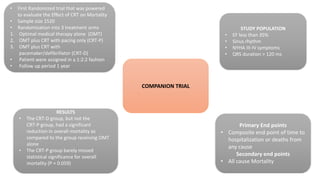
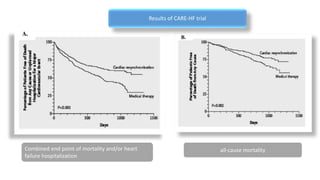
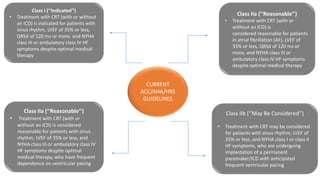
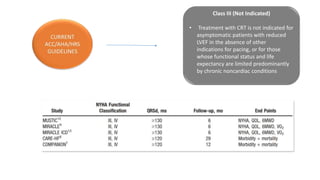
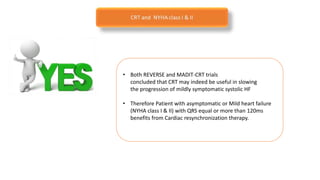
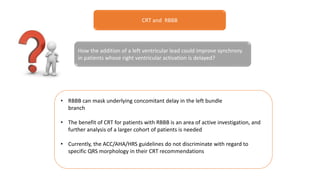
This document summarizes a presentation on cardiac resynchronization therapy (CRT). It discusses how CRT works to restore synchronized heart contraction in patients with heart failure and ventricular dyssynchrony. It reviews several important clinical trials that demonstrated the benefits of CRT in reducing mortality and hospitalization. The document also discusses current guidelines for CRT, factors that can reduce the effectiveness of CRT, and ongoing areas of research around using CRT in populations with narrow QRS or mild heart failure symptoms.