
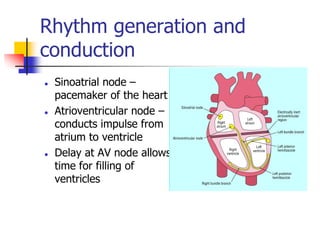
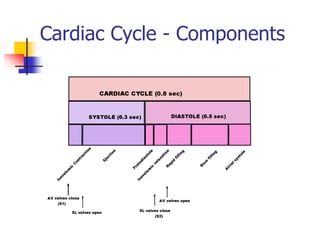
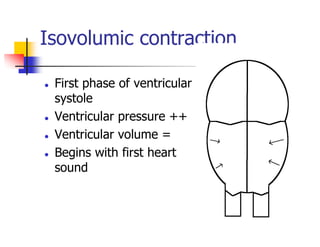
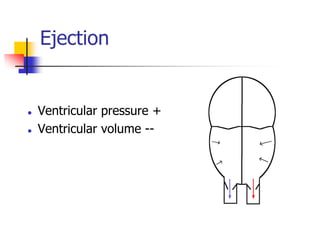
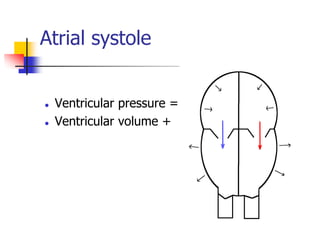
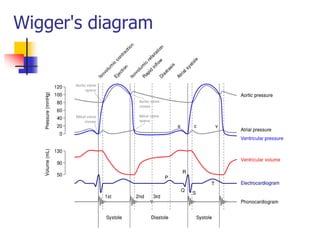
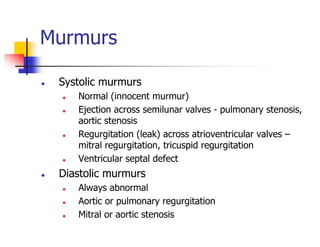
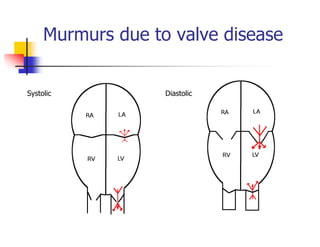
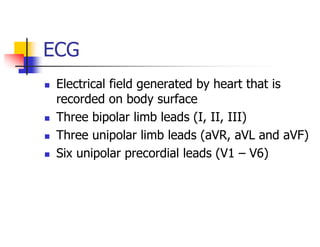
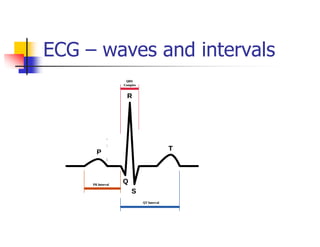
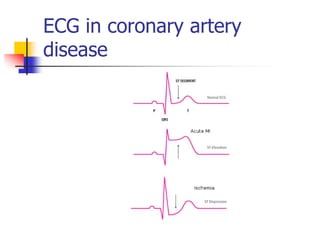

The cardiac cycle consists of rhythmic changes that occur with each heartbeat. It has several phases including isovolumic contraction, ejection, isovolumic relaxation, and atrial systole. Heart sounds are produced by the closing of valves and include S1, S2, S3, S4, and murmurs. An electrocardiogram (ECG) records the electrical activity of the heart through electrodes on the skin and analyzes waves, intervals, and other characteristics to evaluate heart rate and identify conditions like coronary artery disease.














































![[Int. med] heart murmurs from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/b29t6cwrtzwunmrfazue-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)






































