This document discusses channelopathies, focusing on Brugada syndrome and long QT syndrome. It describes:
- The types of channelopathies including Brugada syndrome, long QT syndrome, short QT syndrome, and catecholaminergic polymorphic ventricular tachycardia.
- The ion channel mutations that cause each condition, such as loss of function mutations in SCN5A causing Brugada syndrome and gain of function mutations in SCN5A causing long QT syndrome type 3.
- The clinical features, diagnosis, and management of Brugada syndrome and long QT syndrome. Risk stratification and indications for ICD placement are also covered.



![Brugada Syndrome
■ Inheritable form of idiopathic ventricular arrhythmia
■ Loss Of Functional Mutations in the SCN5A gene [encodes for the α-subunit of the sodium channel]
■ Autosomal Dominant, predominantly in males; presentation at 40yrs
■ Prevalence- 1–5 per 10,000 worldwide [highest in Southeast Asia]
■ Family history of unexplained sudden death
■ ECG:ST-segment elevation in right precordial leads with right bundle branch block-like morphology
■ Increased risk for potentially lethal polymorphic VT or VF
[particularly during sleep in the absence of structural heart disease]](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-5-320.jpg)


![Pathophysiology
■ Loss of INa
■ Increased Ito current [Ito
Epi>>Endo]
■ Reduced in conditions
increasing ICaL currents
(catecholamines),
increasing AP duration](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-8-320.jpg)




![Diagnosis
■ Type 1 pronounced elevation of the J point and coved – type ST-
segment elevation >2 mm changes in > 1 right precordial lead (V1 toV3),
in the presence or absence of a Na channel blocker [Ajmaline, Flecainide,
and Procainamide] and one of the following
1. DocumentedVF
2. Self terminating polymorphicVT
3. Family history of SCD (<45 years)
4. Coved type ECGs in family members
5. Electrophysiological inducibility
6. Syncope
7. Nocturnal agonal respiration.](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-13-320.jpg)


















![Pathophysiology
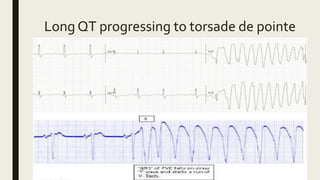
■ EAD (R onT VT)
■ DAD
■ Reentry- TdP
– [HypoK, HypoMg, K blocking
drugs (I, III), bradycardia]](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-32-320.jpg)














![Management
■ Life style modification
■ b blockers in LQTS clinical diagnosis (ecg) [ may be given in patient
with molecular diagnosis alone]
■ PPI in cases with sustained pause dependentVT +/- QT prolongation
■ ICD in survivors of cardiac arrest, may be given in b blocker resistant,
considered in high risk groups [LQT2, LQT3, QT>500ms]
[Left cardiac sympathetic denervation considered for symptomatic b
blocker resistant]](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-47-320.jpg)








![Pathophysiology
5 genes
Gain of function mutations in K channel-
KCNH2 [IKr] (SQT1),
KCNQ1 [IKs] (SQT2),
KCNJ2 [IK1] (SQT3)
Loss of function mutations in ICaL –
CACNA1C (SQT4)
CACNB2b (SQT5)
•Atrial & Ventricular-very short
APD & RP vulnerable to reentry
& easily inducible.
•Relatively prolonged T peak-T end
interval suggesting augmented
transmural dispersion of
repolarization](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-57-320.jpg)















![Management
■ Risk stratification is based entirely on
clinical considerations.
■ Regular follow-up visits, TMT constitute
an effective approach for B-blocker dose
titration and arrhythmia monitoring
■ Holter monitoring [sometimes acute
emotions ppt]
■ Mainstay of Management B-Blockers
[long term follow up 40% have
symptom recurrence]
■ ICD in B-blocker ineffective cases or
survivor of Cardiac arrest](https://image.slidesharecdn.com/channelopathieslecture-180222140259/85/Cardiac-Channelopathies-73-320.jpg)




































































