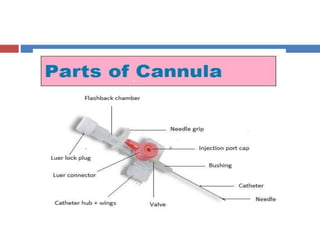
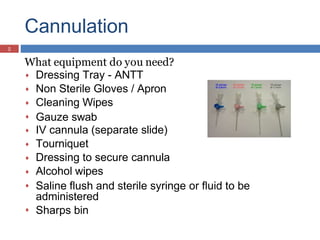
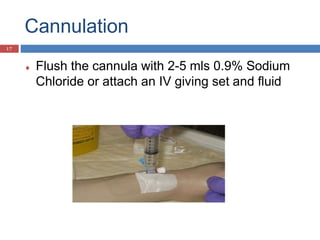
This document provides information on intravenous cannulation including indications, advantages, necessary equipment, preparation, procedure, possible complications, and site selection considerations. The procedure involves identifying a suitable vein, cleaning the site, inserting the cannula at a 10-30 degree angle, observing for flashback, advancing the cannula over the needle while withdrawing, securing it with a dressing, and flushing it with saline. Potential complications include infection, cellulitis, infiltration if fluid leaks into tissue, and thrombophlebitis. Proper technique and assessment of vein characteristics can help minimize risks.