Downloaded 101 times

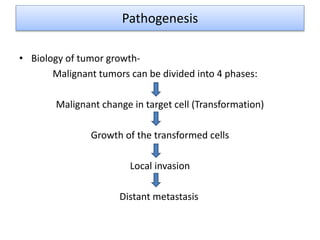

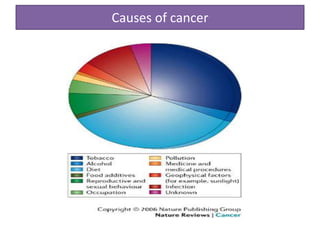
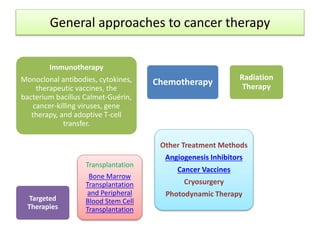






This document serves as a comprehensive research guide on cancer, detailing its incidence, pathogenesis, causes, diagnosis, treatment methodologies, and recent advances in the field. It describes different types of cancers, their pathological classification, and the biological mechanisms driving tumor growth, as well as the various approaches to treatment, including chemotherapy and targeted therapies. Additionally, it outlines future trends in cancer research aiming to improve therapeutic effectiveness and reduce toxicity.




















































































