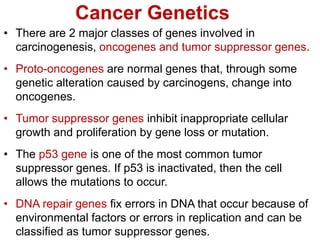
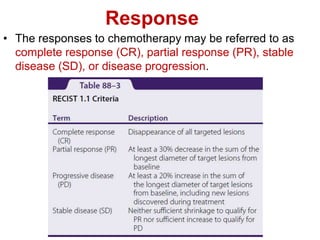
Cancer chemotherapy and treatment involves several methods. Chemotherapy uses drugs to prevent or treat cancer by killing cancer cells. Common chemotherapies include fluorouracil, capecitabine, and cytarabine which are pyrimidine analogues that interfere with DNA synthesis in cancer cells. These drugs have similar mechanisms of action but different routes of administration and toxicity profiles. Combination chemotherapy uses multiple agents to increase effectiveness while reducing resistance. Careful dosing and administration is needed due to the narrow therapeutic index of chemotherapy drugs.
![Cont…
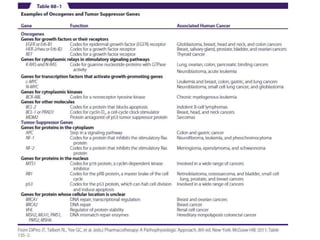
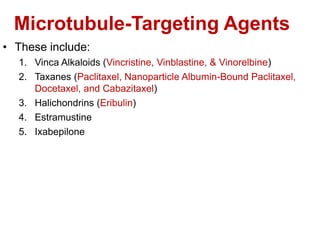
• The dose density of chemotherapy refers to shortening of
the period between cycles of chemotherapy.
• This can accomplish 2 things: 1st, the tumor has less time
between cycles of chemotherapy to grow, & 2nd, patients
receive the total number of required cycles in a shorter
time period.
• Administration of dose-dense chemotherapy regimens
often requires the use of colony-stimulating factors (eg,
filgrastim or granulocyte colony-stimulating factor [G-CSF])
to be administered; These agents shorten the duration and
severity of neutropenia.](https://image.slidesharecdn.com/anticancer-231114130743-635262ff/85/ANTICANCER-ppt-24-320.jpg)












































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
