This document discusses cancer of the vulva, including its incidence, risk factors, types, diagnosis, staging, prognosis, and management. Some key points:
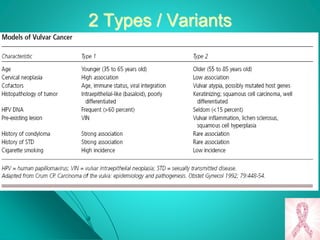
- Vulvar cancer accounts for 1-4% of gynecological cancers and predominantly affects postmenopausal women. Risk factors include HPV infection, smoking, and history of other gynecological cancers.
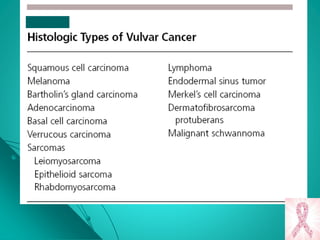
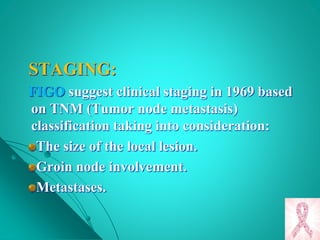
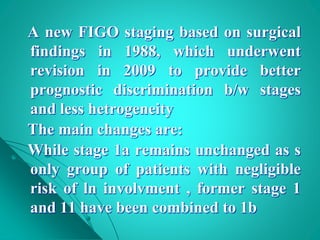
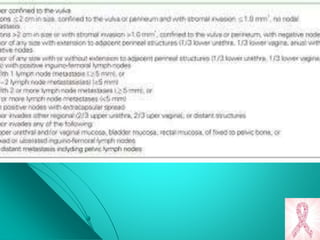
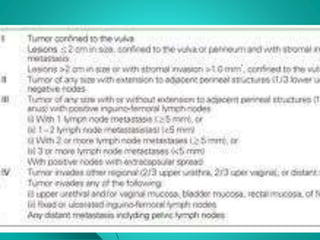
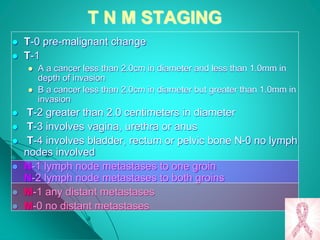
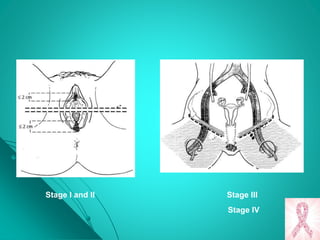
- Squamous cell carcinoma makes up 90% of cases. Diagnosis requires biopsy of any suspicious lesions. Staging is based on tumor size and spread to lymph nodes or distant sites.
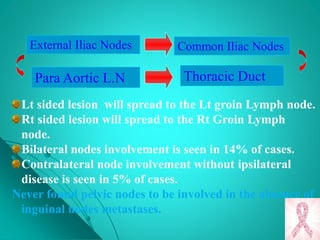
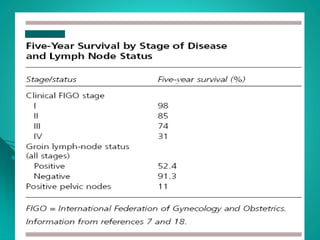
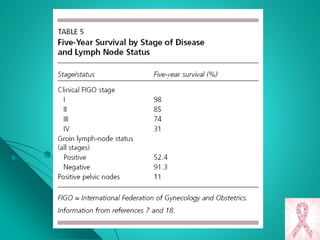
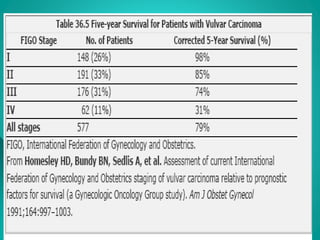
- Prognosis depends on lymph node involvement, with 5-year survival rates over 90% for stage I but under 50% if nodes are



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
