












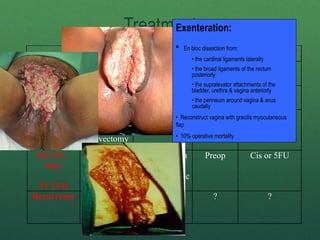

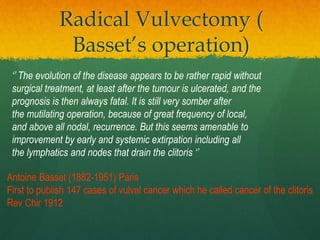


Dr. Jean Peiffer - Wide excision of vulva and perineum - Bilateral inguinal lymphadenectomy - Primary closure - Mortality <5% - Recurrence <10% - Standard treatment for >50 years - Morbidity high: wound breakdown, lymphedema, sexual dysfunction - Replaced by less radical surgery when LN status shown to be most important prognostic factor - Still indicated for large fixed tumors with close or positive margins - Adjuvant radiation reduces recurrence rates - Quality of life better with less radical surgery when oncologically sound - Basset’s operation established vulvar cancer surgery as a subspecial