Download as PDF, PPTX


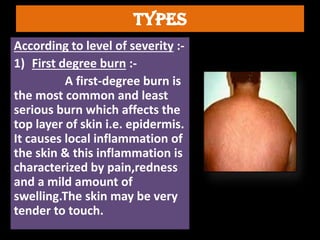
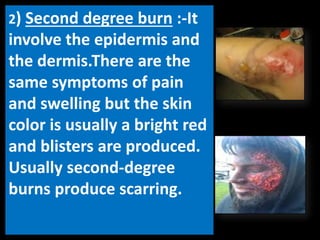
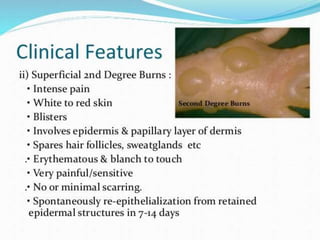
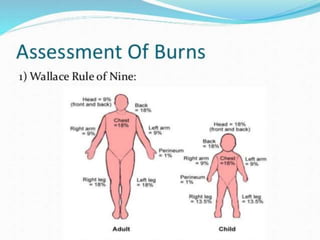
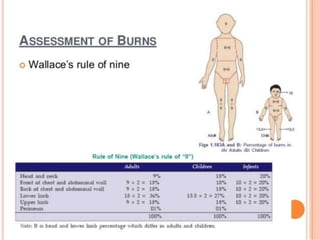
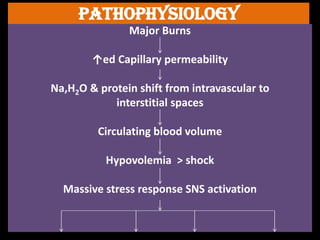
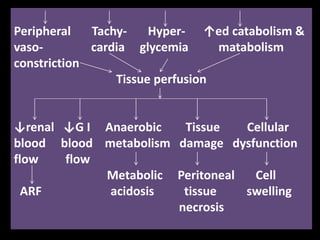








Burns are injuries to the skin or other tissues caused by heat, flames, chemicals, electricity, or radiation. There are three degrees of burns - first degree involves only the outer layer of skin, second degree extends deeper into the layers of skin, and third degree burns are the most severe and destroy both the outer and deeper layers of skin. Proper burn management includes assessing the severity of the burn, giving intravenous fluids to prevent shock, cleaning and dressing the wound, providing pain medications, and carrying out surgical procedures such as excision and grafting for deep burns.








































![Burn sseminar [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/burnsseminarautosaved-190206163731-thumbnail.jpg?width=640&height=640&fit=bounds)














































