Downloaded 734 times





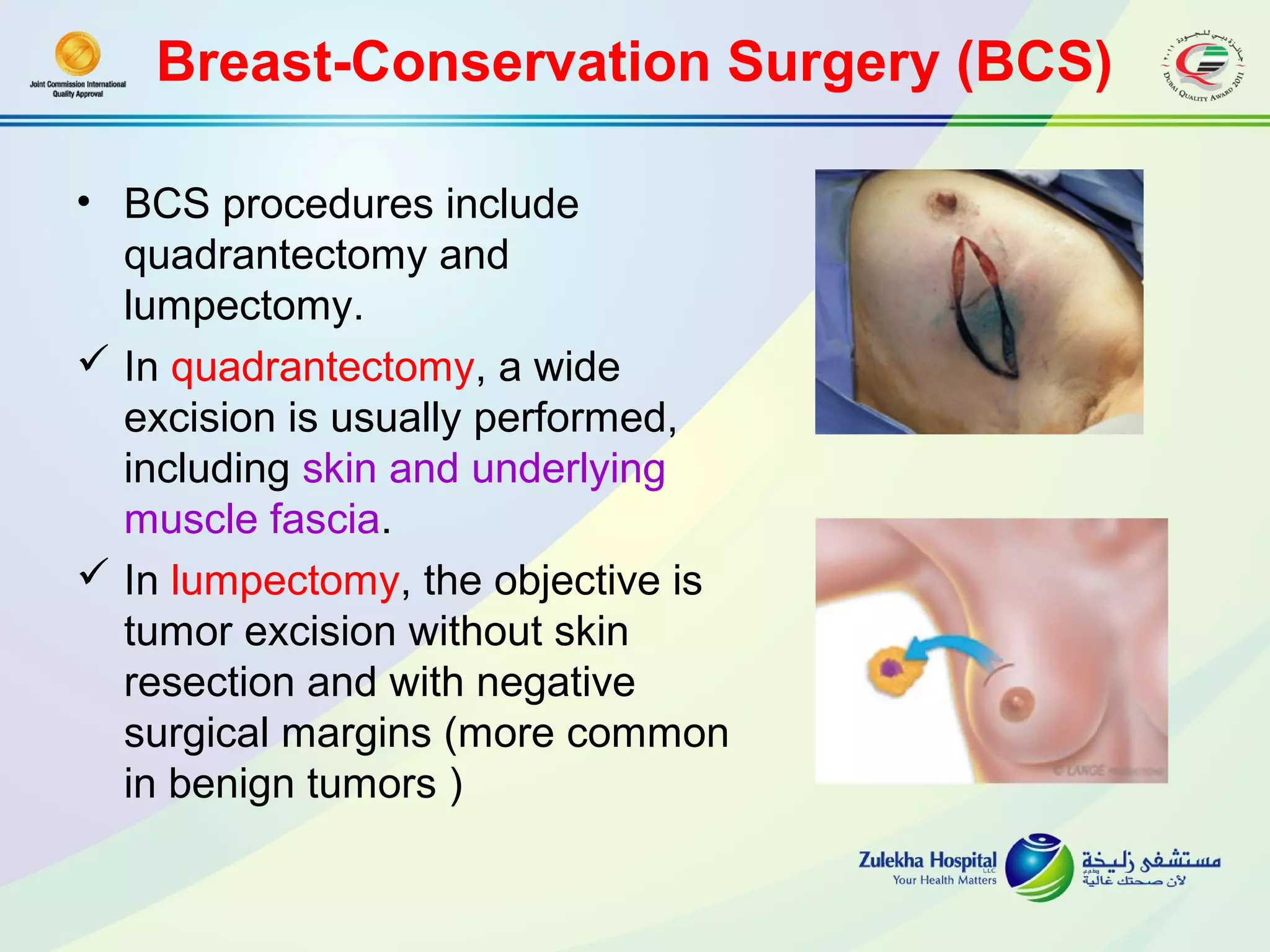
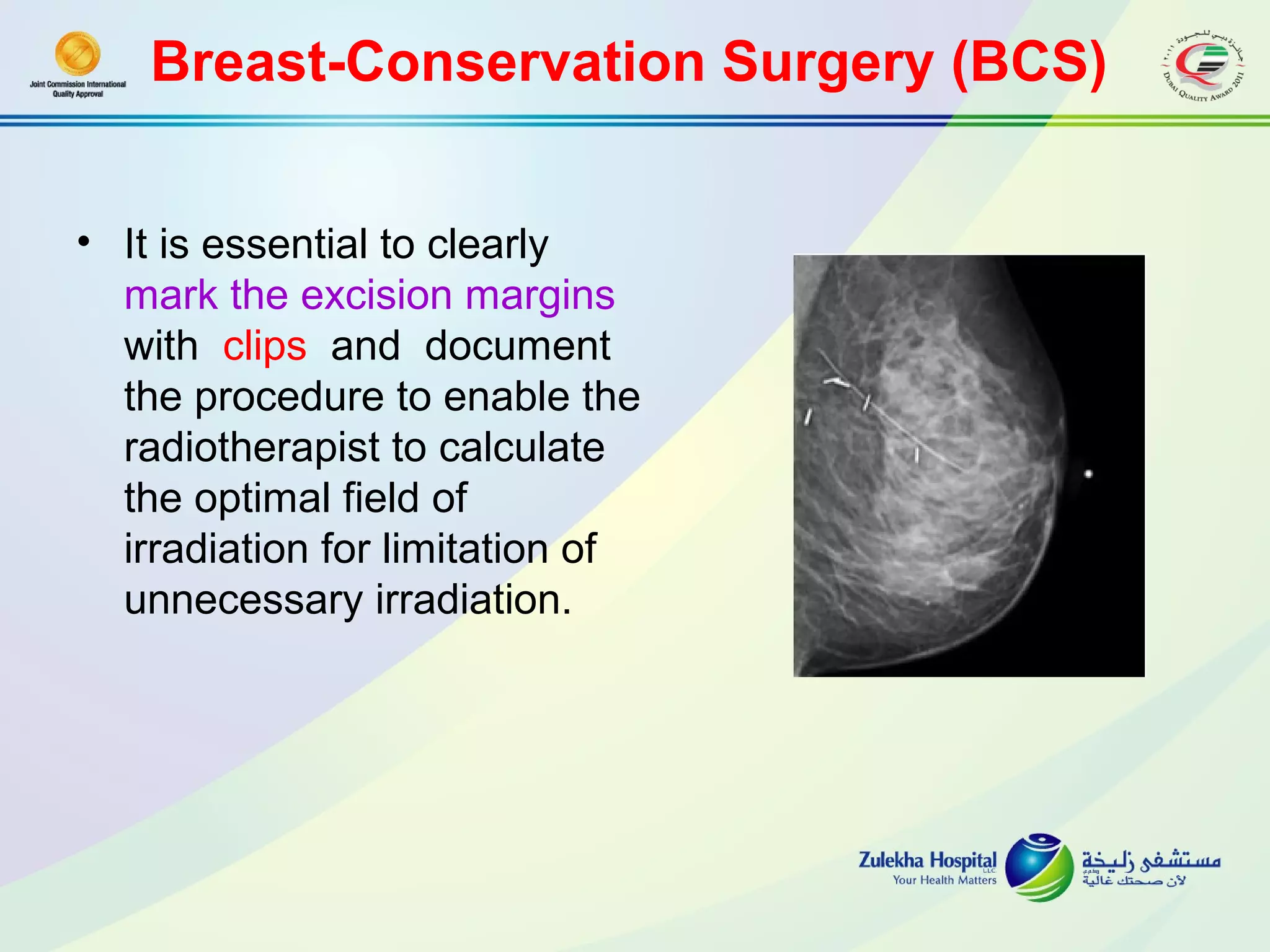















































































































This document discusses oncoplastic breast surgery techniques. It begins by explaining breast conserving treatment and its goals of providing survival equivalent to mastectomy while achieving low recurrence rates. It then discusses various breast conserving surgery procedures like lumpectomy and quadrantectomy. The document focuses on the compromise between wide excision margins and satisfactory aesthetic results in breast conserving surgery. It also discusses various reconstruction techniques used after breast conserving surgery, including breast implants, fat grafting, flap procedures, and oncoplastic breast reconstruction. The principles and mechanisms of oncoplastic surgery are explained. Techniques for peripheral and central tumors are classified.



































































