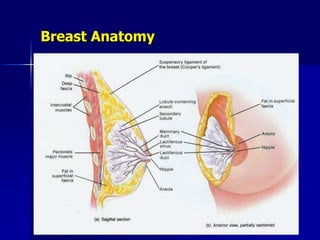
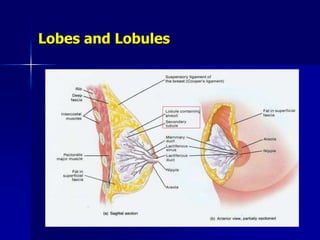
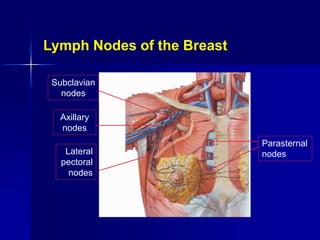
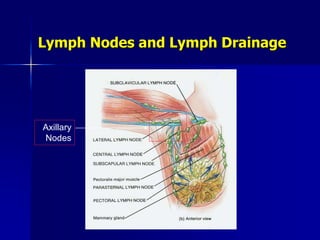
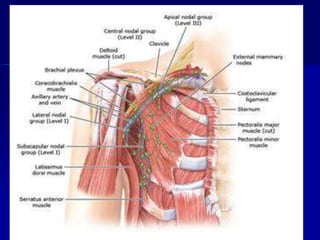
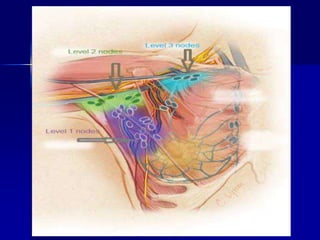
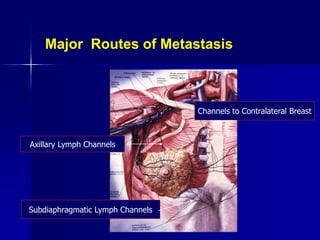
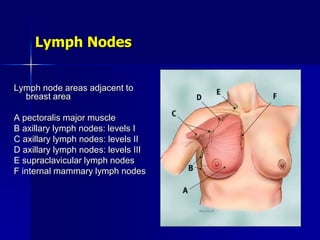
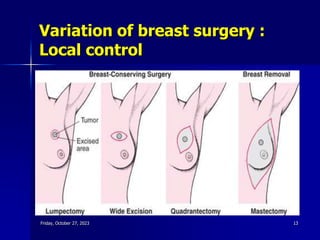
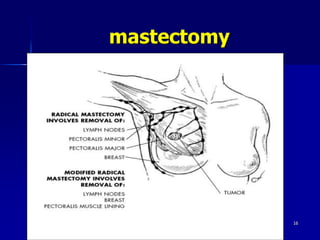
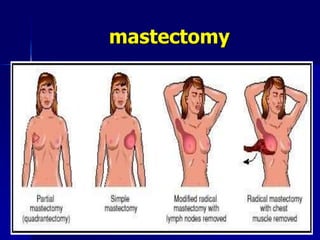
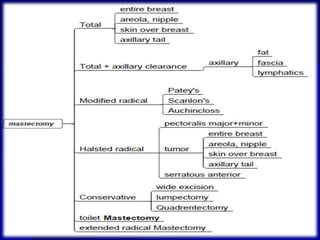
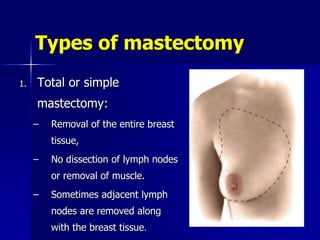
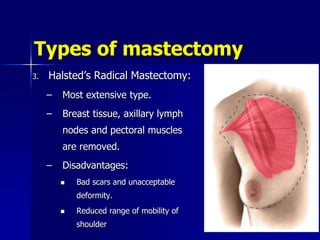
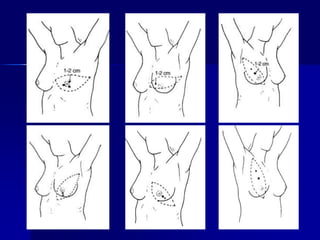
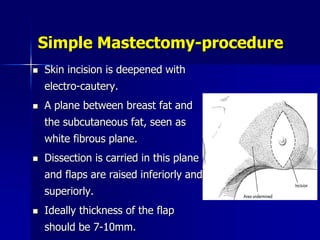
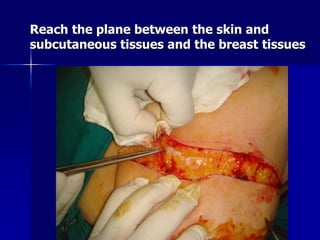
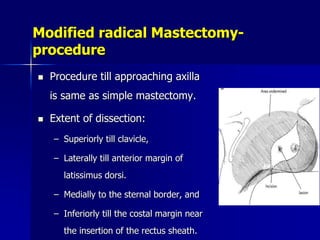
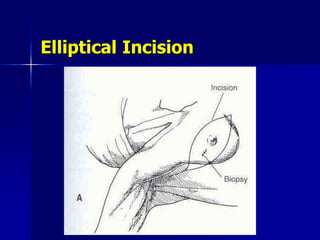
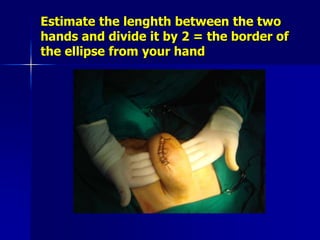
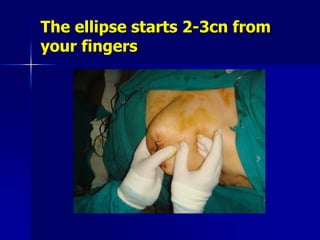
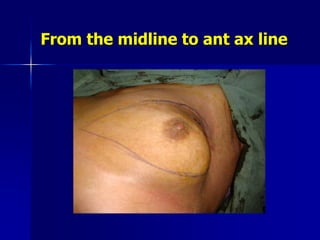
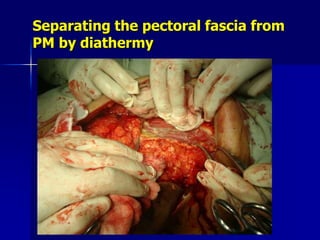
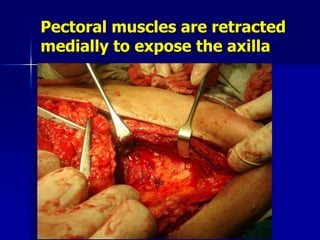
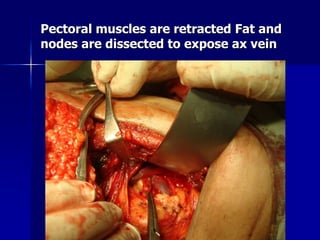
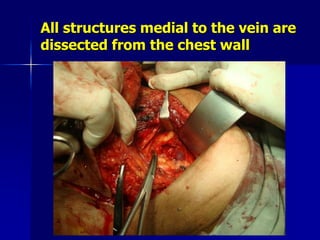
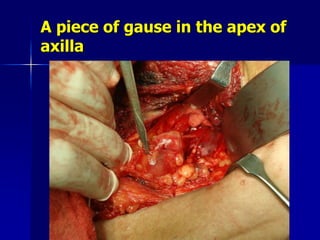
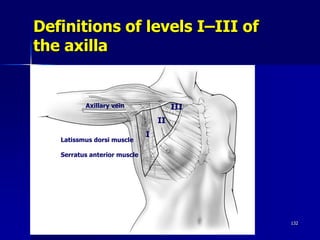
This document discusses different types of mastectomy procedures for breast cancer treatment. It begins by describing breast anatomy and lymph node drainage patterns. It then covers the different types of mastectomies including simple/total mastectomy, modified radical mastectomy, radical mastectomy, and skin-sparing mastectomy. For each procedure, it provides details on the tissues removed and surgical technique. Indications for mastectomy versus breast conservation are also reviewed.