Downloaded 164 times
![POSTERIOR CANAL BPPVPOSTERIOR CANAL BPPV
Most common– posterior canal is most gravity
dependant in upright and supine position
Once debris enter the post. canal ,the cupula at the
shorter most dependant arm trap the debris.
Debris can exit only through the longer arm through the
crus commune [non-ampullary]](https://image.slidesharecdn.com/bppvandparticlerepositioningmaneuvers-150212072357-conversion-gate02/85/Bppv-and-particle-repositioning-maneuvers-6-320.jpg)

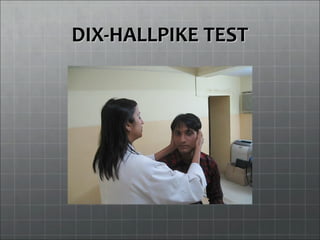
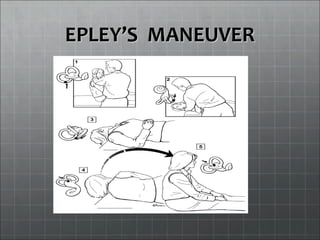
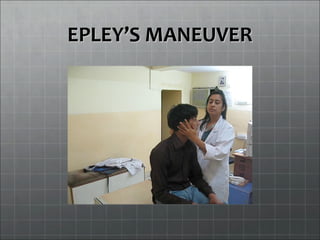


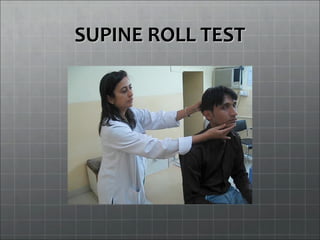
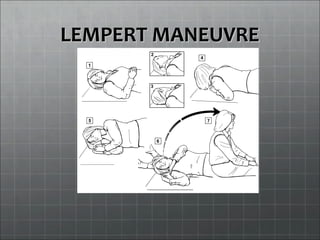
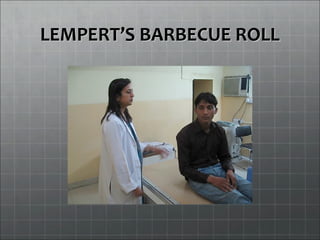
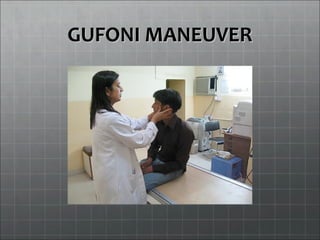

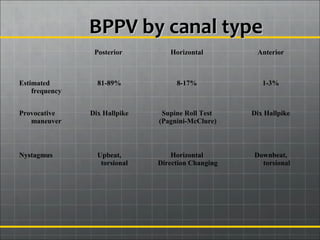
This document discusses benign paroxysmal positional vertigo (BPPV), including its causes, types, diagnostic tests, and treatment maneuvers. It provides details on: - Posterior canal BPPV is the most common type, accounting for 81-89% of cases. The Dix-Hallpike test is used for diagnosis. Treatment includes particle repositioning maneuvers like Epley's maneuver. - Horizontal canal BPPV, which accounts for 8-17% of cases, is diagnosed using tests like the supine roll test. Treatments include maneuvers like the Lempert maneuver. - Anterior canal BPPV is rare but can result from treatments for other forms















































































