Downloaded 15 times

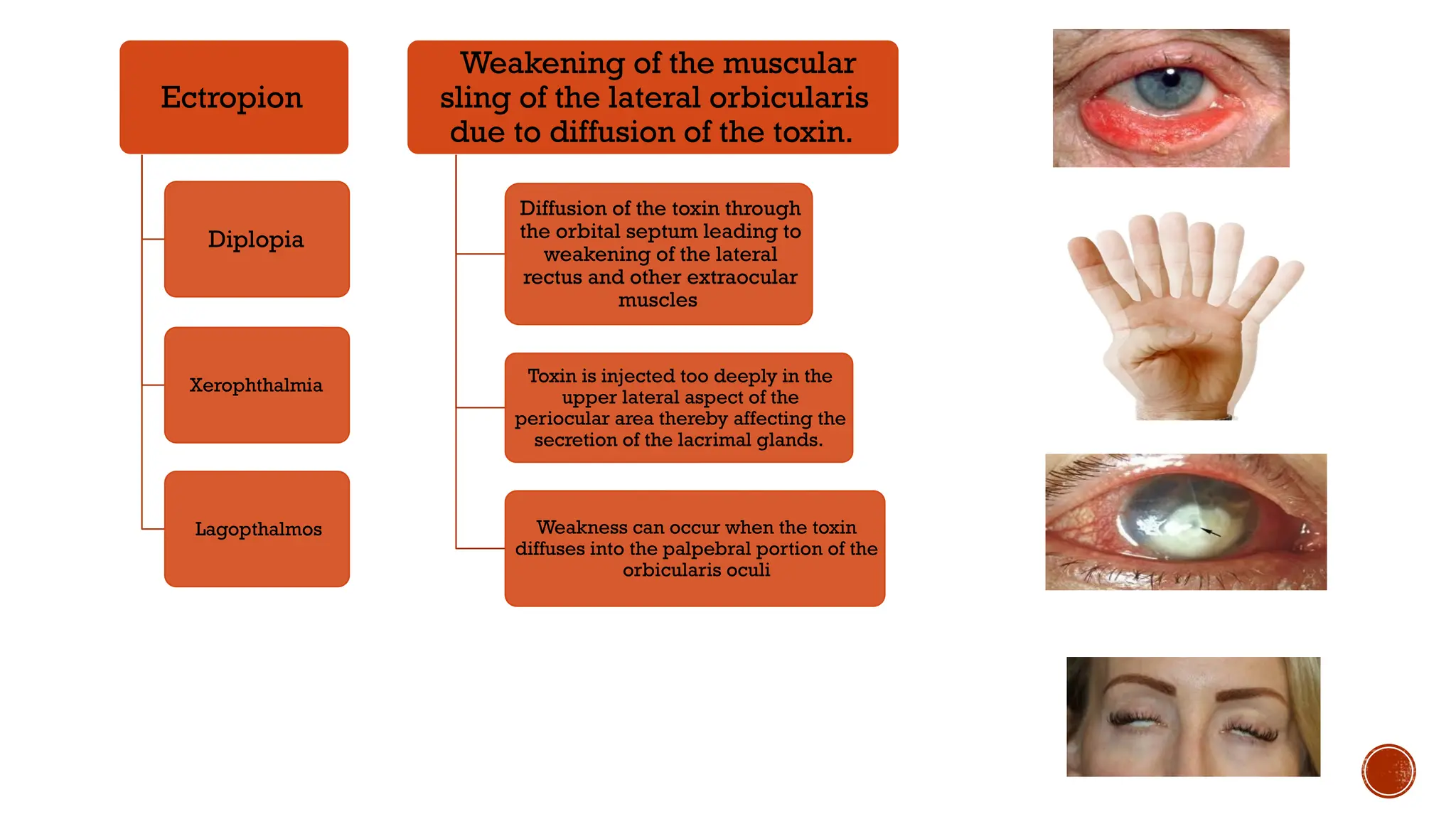
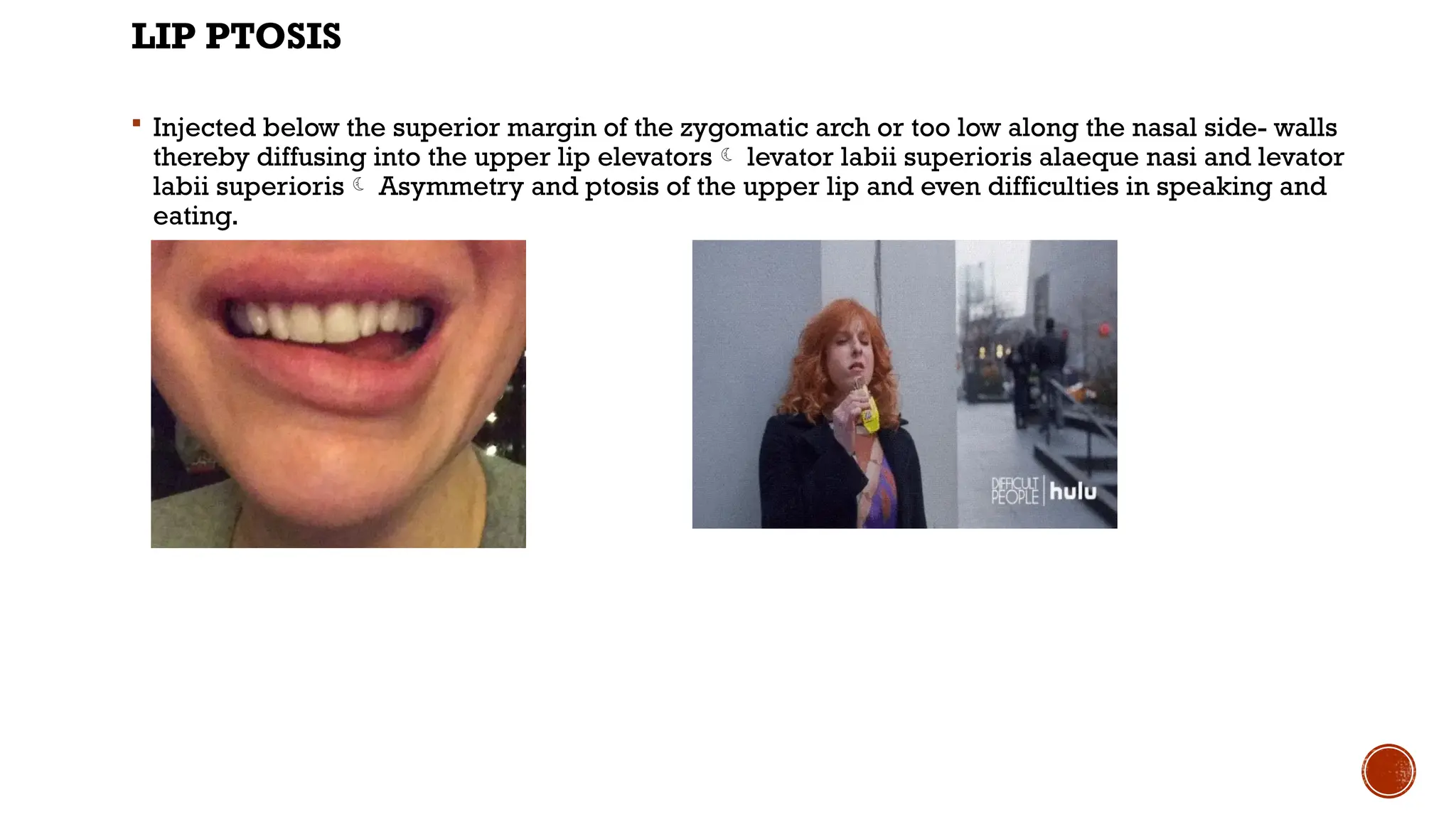
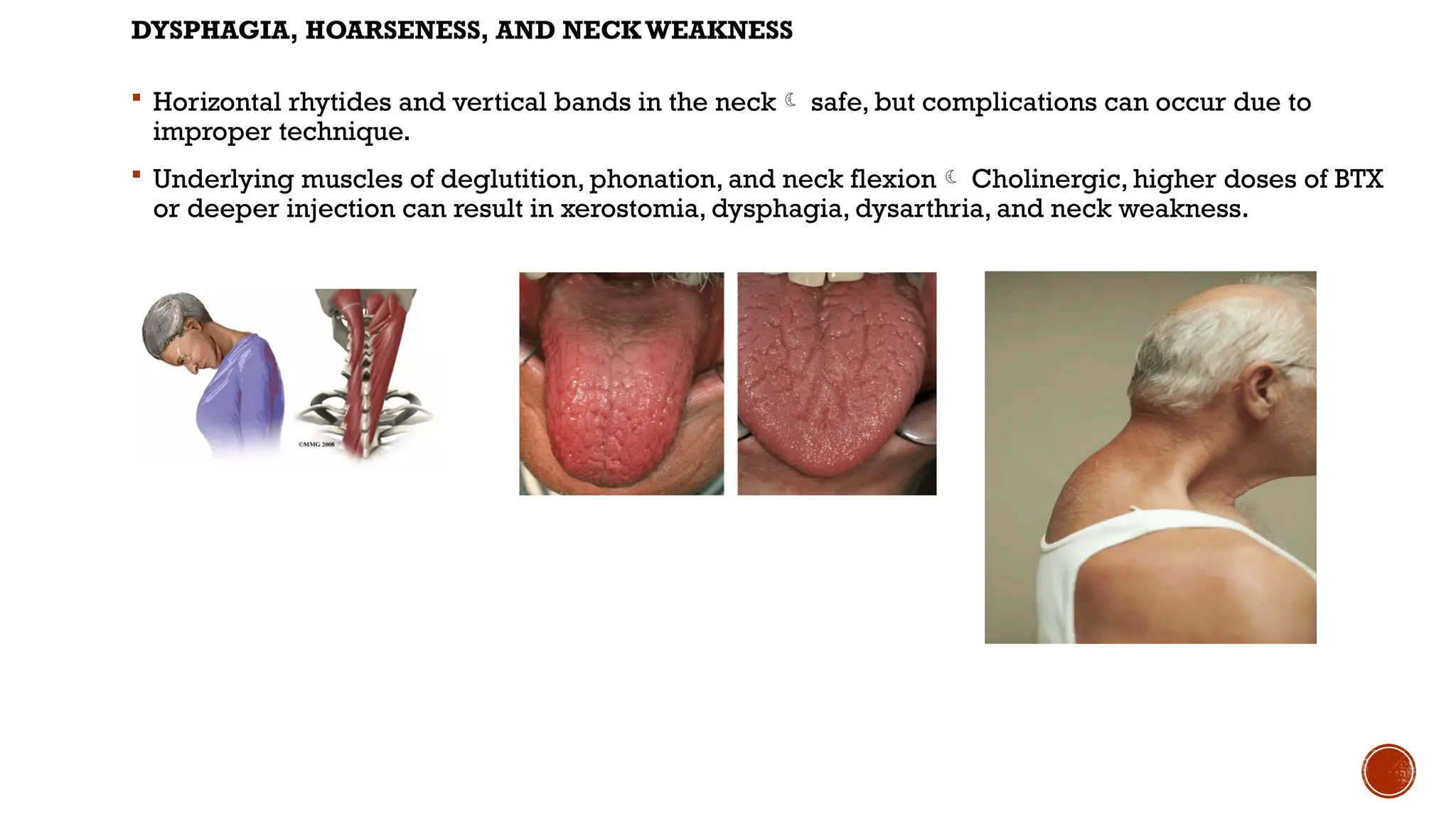
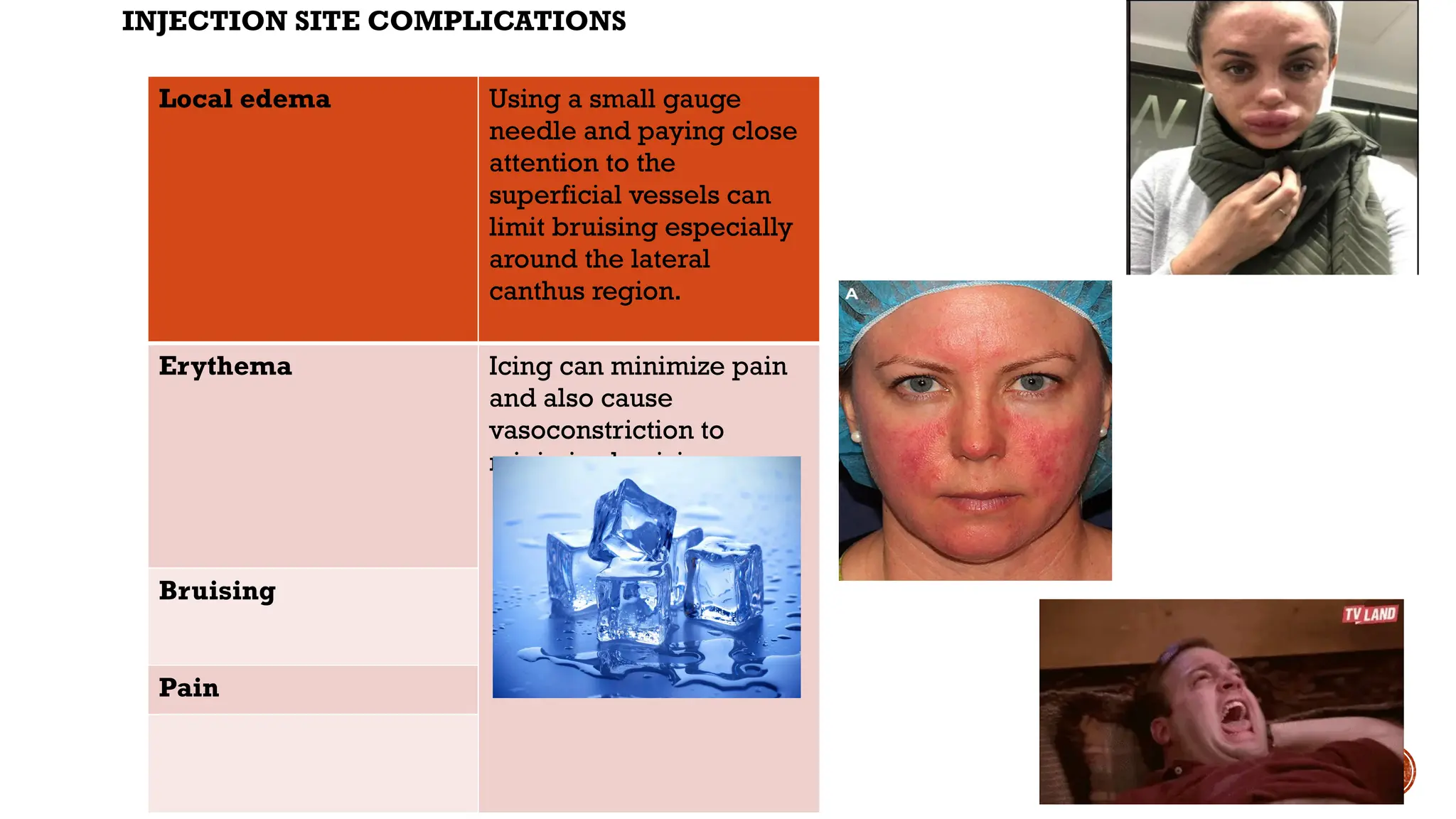
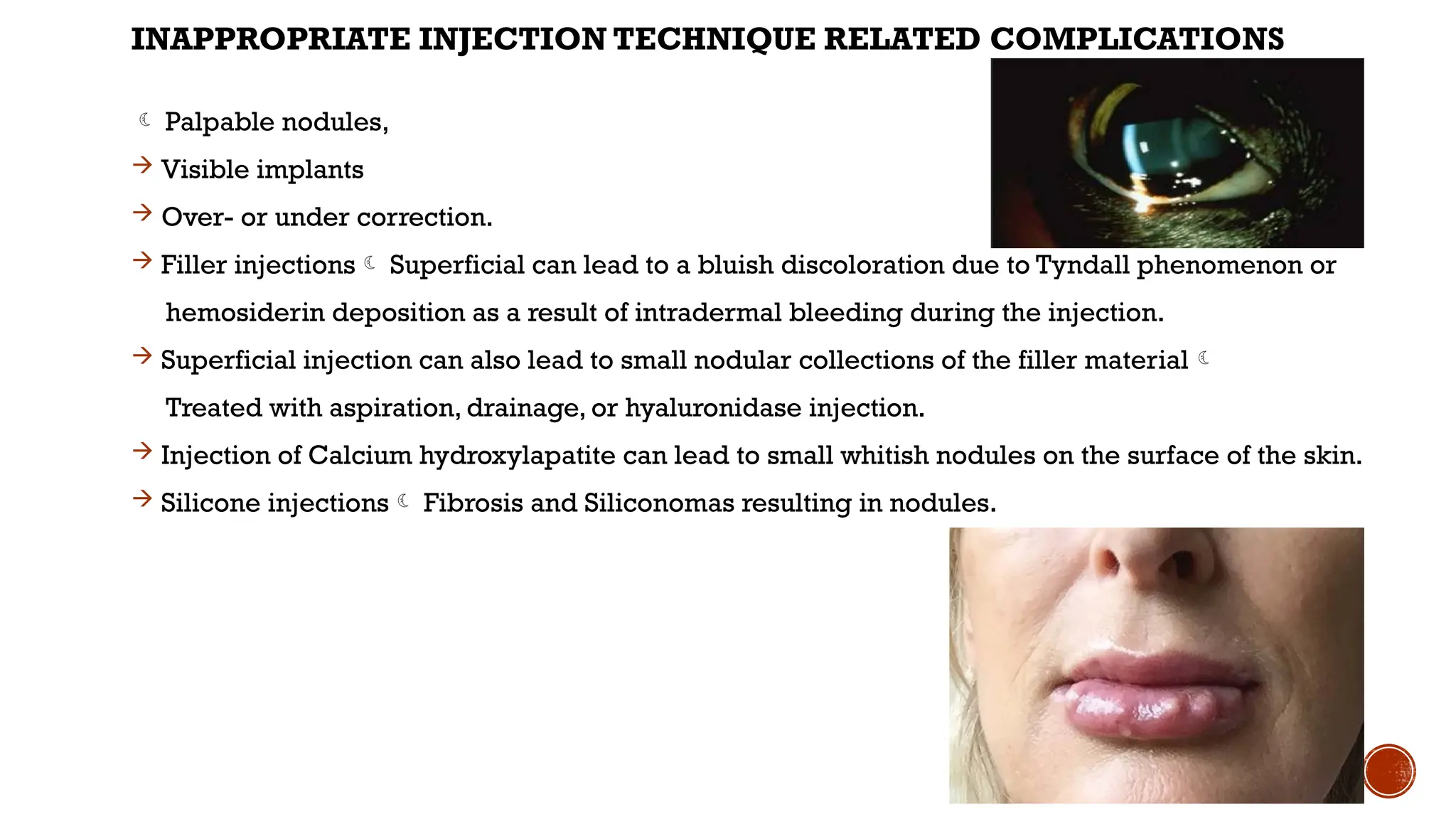
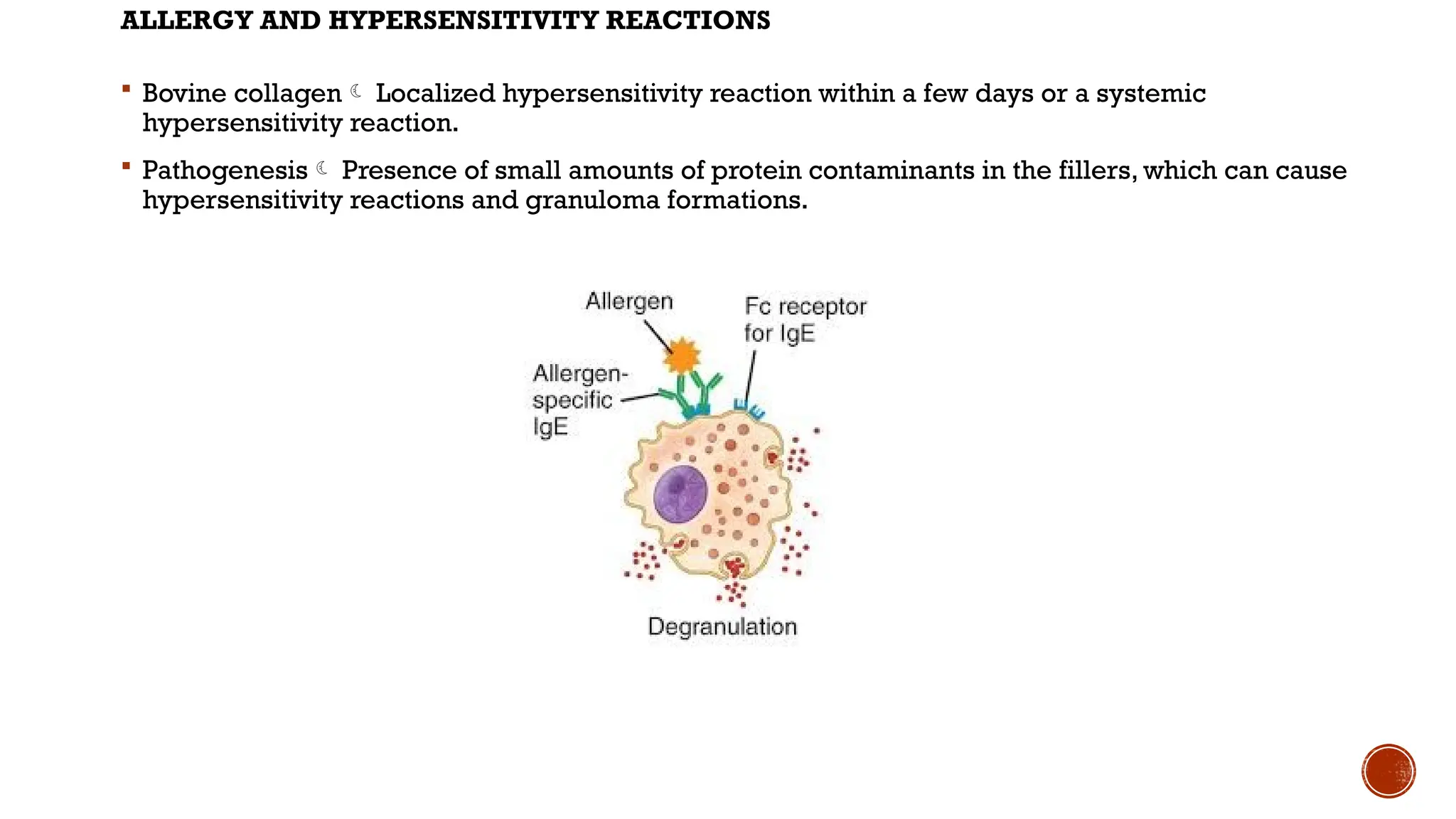
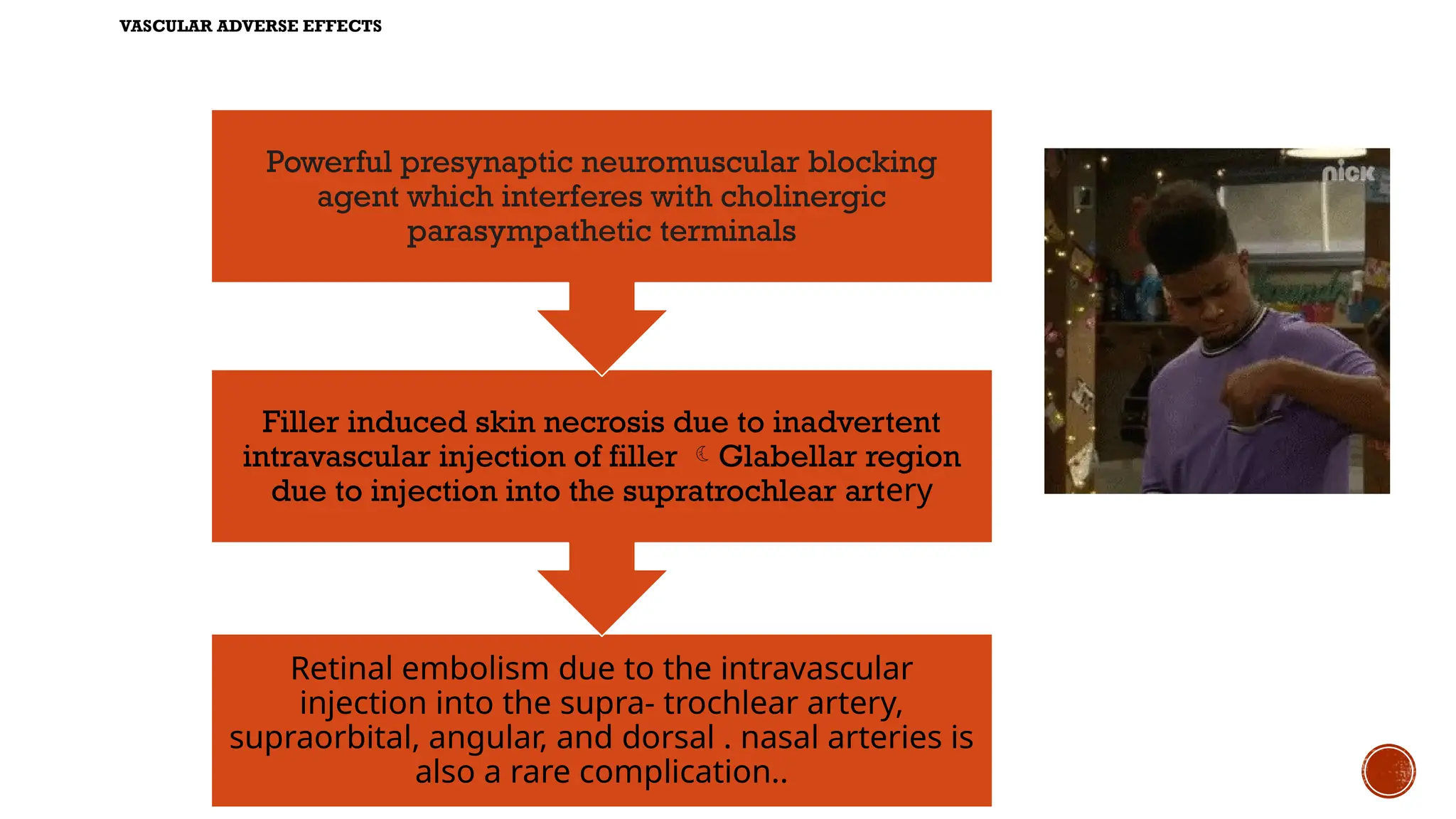


The document discusses the risks and complications associated with Botox and other cosmetic procedures, emphasizing the importance of patient selection and thorough consultation to prevent dissatisfaction and complications. It outlines potential issues such as facial asymmetry, ptosis, allergic reactions, and vascular complications, while also addressing contraindications and necessary precautions during treatment. Additionally, it highlights the importance of proper injection techniques to minimize risks and ensure patient safety.



























![Scalp[1]](https://cdn.slidesharecdn.com/ss_thumbnails/scalp1-170504174806-thumbnail.jpg?width=640&height=640&fit=bounds)



















![Treatment of periorbital_rhytids_with_botox[1]](https://cdn.slidesharecdn.com/ss_thumbnails/treatmentofperiorbitalrhytidswithbotox1-130422140956-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































