Ch 185 - Cosmetic Uses of Botox and Injectable Fillers.ppt
1.
Cosmetic Uses ofBotox and
Injectable Fillers
Andrew Morrissey
June 17, 2008
2.
Introduction
Botox isbest used to eliminate or soften dynamic
facial lines (wrinkles that appear with active
contraction of the facial muscles)
Fillers are used to help efface facial wrinkles or
creases that are apparent at rest.
Botox can help prevent facial wrinkles from
developing or deepening
Fillers are used for the treatment of already
established rhytids.
The combination of the two products together
often give a better result than either product alone.
3.
Anatomy
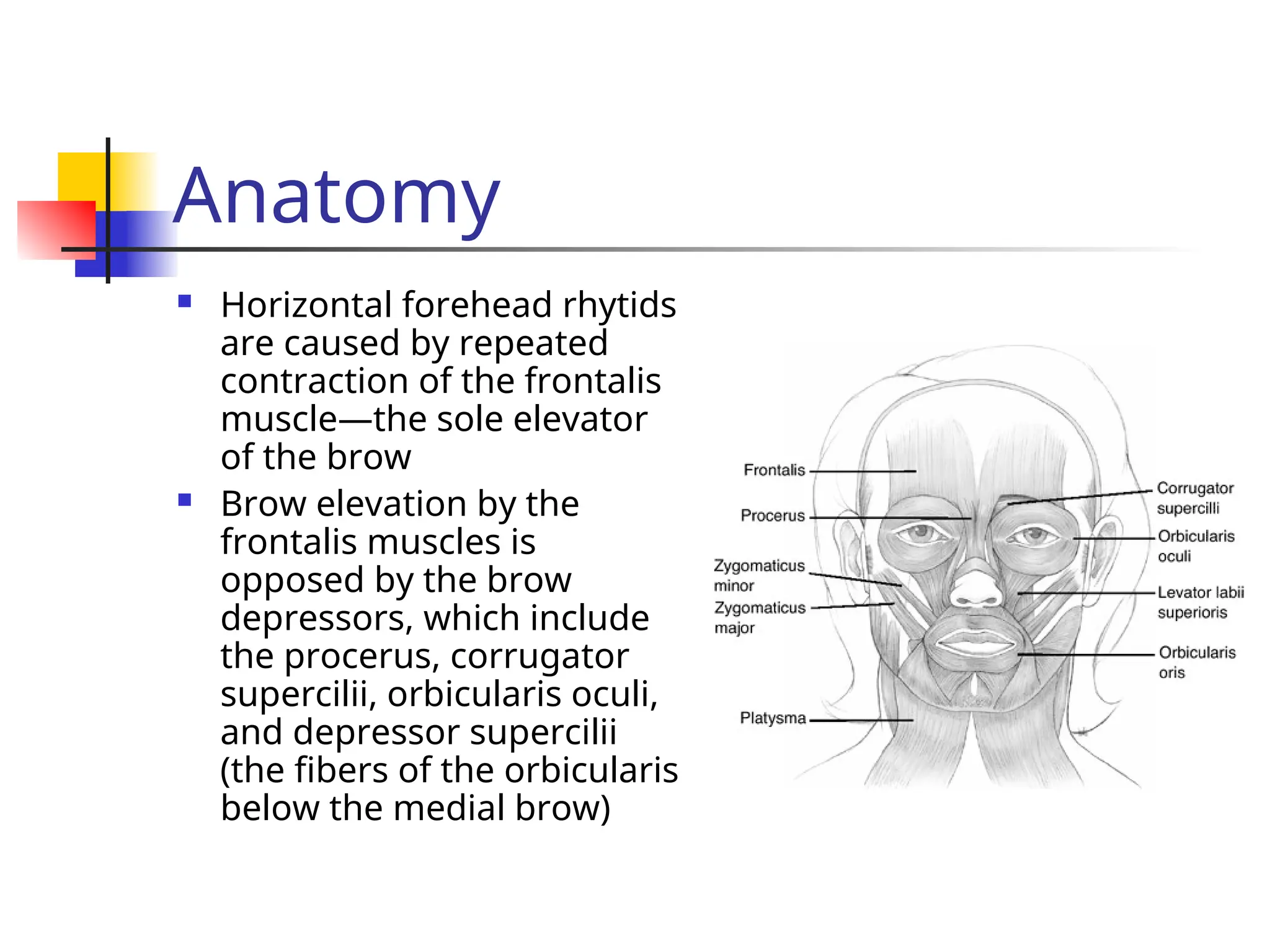
Horizontal foreheadrhytids
are caused by repeated
contraction of the frontalis
muscle—the sole elevator
of the brow
Brow elevation by the
frontalis muscles is
opposed by the brow
depressors, which include
the procerus, corrugator
supercilii, orbicularis oculi,
and depressor supercilii
(the fibers of the orbicularis
below the medial brow)
4.
Anatomy
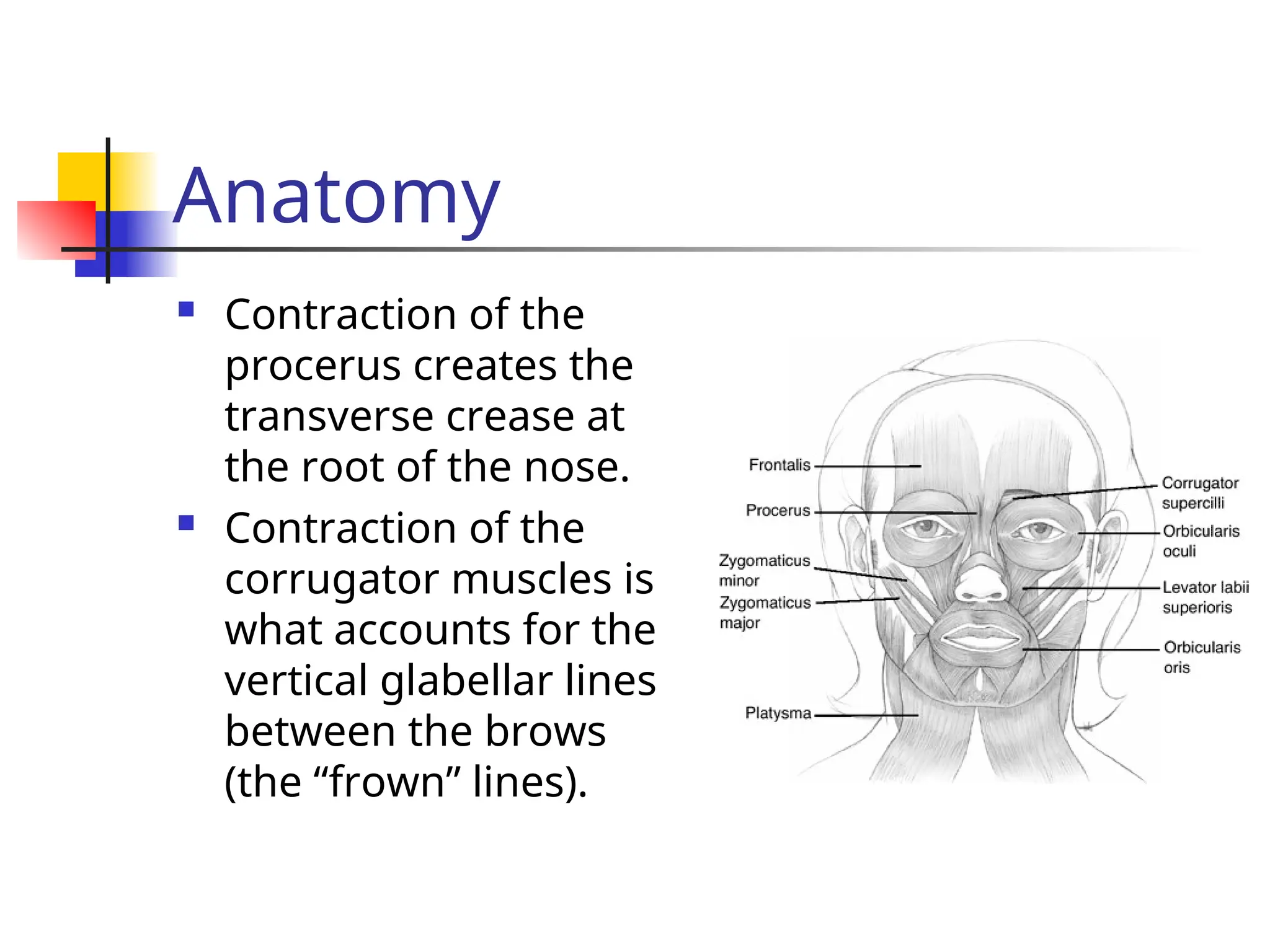
Contraction ofthe
procerus creates the
transverse crease at
the root of the nose.
Contraction of the
corrugator muscles is
what accounts for the
vertical glabellar lines
between the brows
(the “frown” lines).
5.
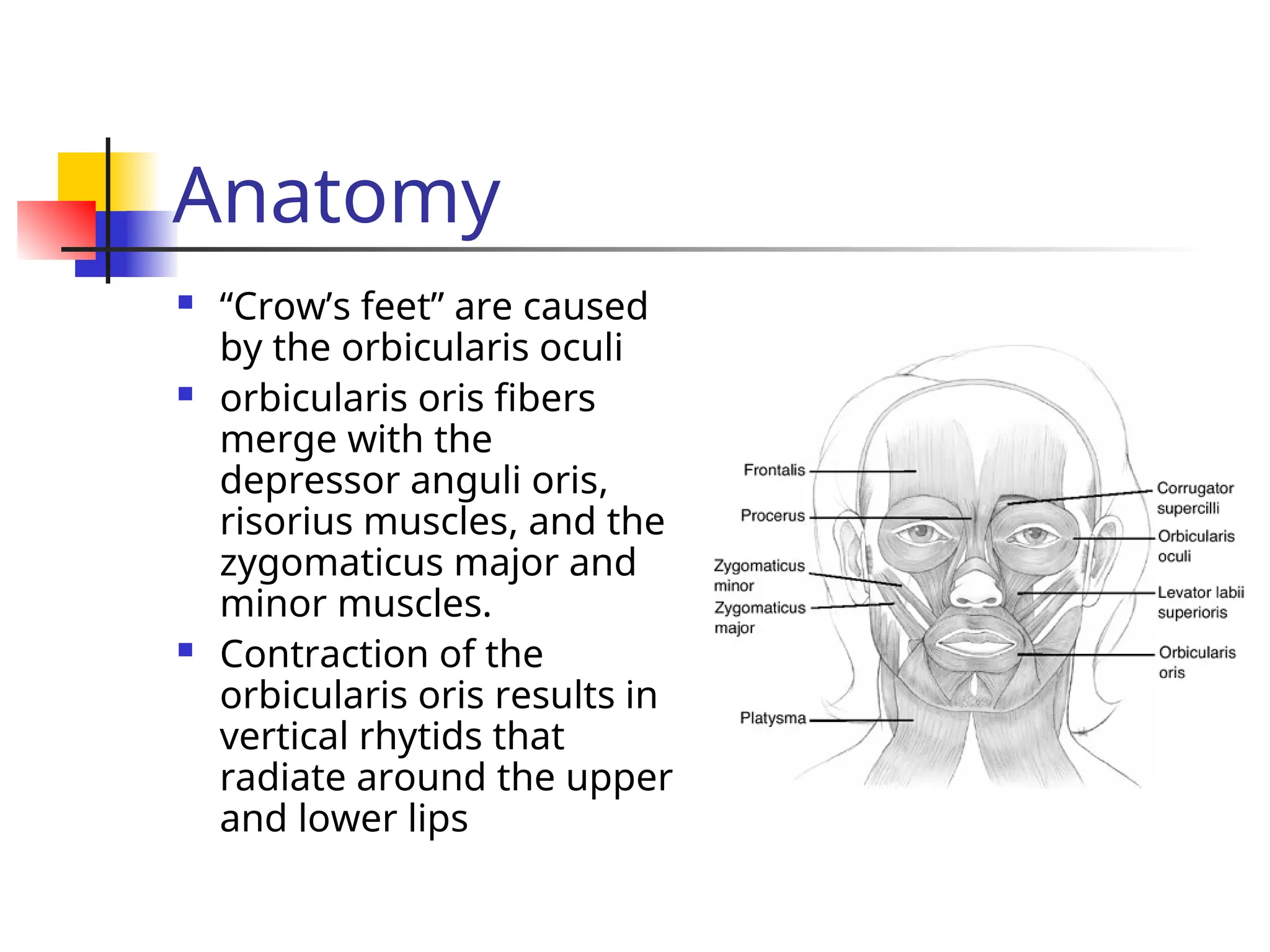
Anatomy
“Crow’s feet”are caused
by the orbicularis oculi
orbicularis oris fibers
merge with the
depressor anguli oris,
risorius muscles, and the
zygomaticus major and
minor muscles.
Contraction of the
orbicularis oris results in
vertical rhytids that
radiate around the upper
and lower lips
6.
Botox – Mechanismof
Action
Botulinum toxin A is produced by the anaerobic bacterium
Clostridium botulinum.
It produces 8 antigenically distinct neurotoxins, 7 are
neuroparalytics.
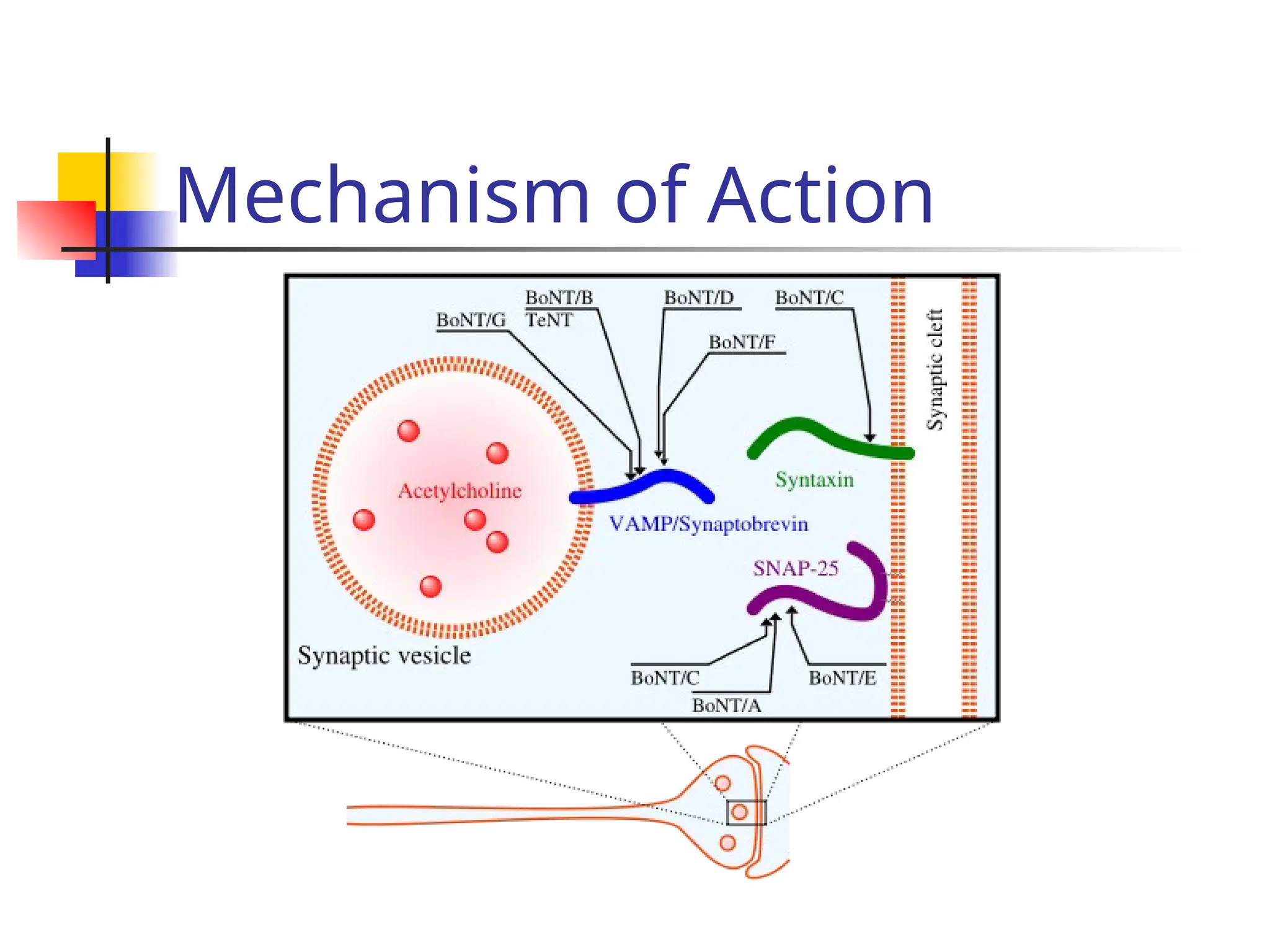
The toxin produces a temporary chemical denervation by
inhibiting the release of acetylcholine from the presynaptic
neuron at the motor endplates of a voluntary muscle.
The paralysis is temporary because chemodenervation is
followed by the growth and sprouting of new axonal
collaterals, which establish new connections at the motor end
plate.
At about 3 months, neural transmission is reestablished, and
the collateral axons regress
Hence clinical efficacy is typically 3-4 months.
Indications/usage
Botox iscurrently approved for use in cervical
dystonia, strabismus, blepharospasm and for the
temporary improvement in vertical glabellar rhytids.
Many “off-label” uses
Botox use is contraindicated in individuals with
preexisting neuromuscular disorders (e.g.,
myasthenia gravis, amyotrophic lateral sclerosis,
Eaton-Lambert syndrome) and those with an
albumin allergy.
Use in pregnancy or lactating mothers is not
recommended… no data
9.
Botox
Supplied ina crystalline form as 100-unit vials.
Dilution with 2.5 mL of preservative-free normal saline
yields a concentration of 4 units per 0.1 ml.
The volume of dilution can vary with the clinician's
preference, but high concentration–low volume injections
help minimize unwanted dispersion into surrounding
tissues.
According to the product info, once reconstituted, it
should be used within 4hrs; many clinicians have
refrigerated any unused toxin for up to 30 days
Following injection, the onset of muscle weakness occurs
between 2 to 5 days, and lasts 3 to 4 mths… full recovery is
noted
10.
Glabellar rhytids
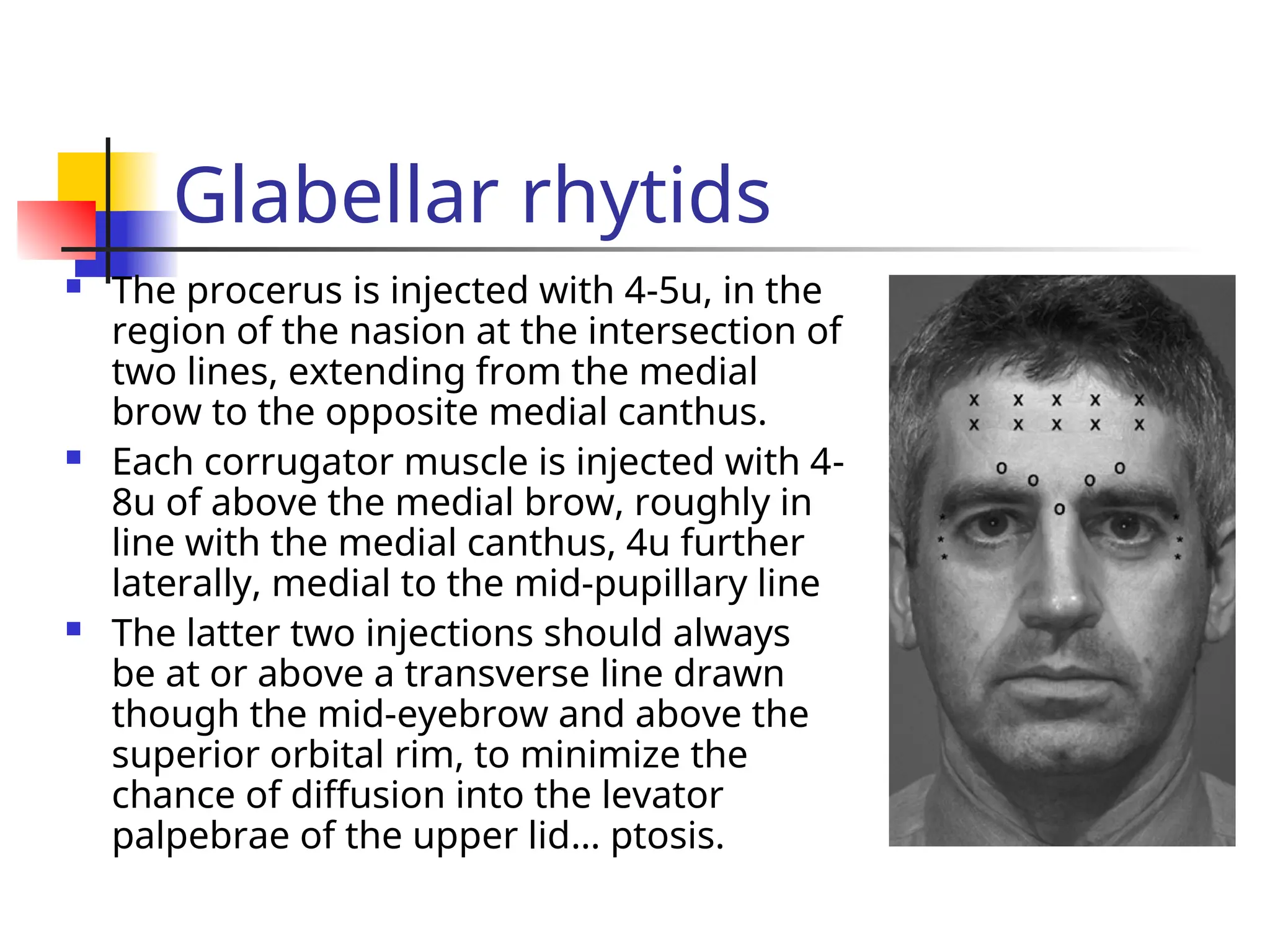
Theprocerus is injected with 4-5u, in the
region of the nasion at the intersection of
two lines, extending from the medial
brow to the opposite medial canthus.
Each corrugator muscle is injected with 4-
8u of above the medial brow, roughly in
line with the medial canthus, 4u further
laterally, medial to the mid-pupillary line
The latter two injections should always
be at or above a transverse line drawn
though the mid-eyebrow and above the
superior orbital rim, to minimize the
chance of diffusion into the levator
palpebrae of the upper lid… ptosis.
11.
Transverse Forehead Rhytids
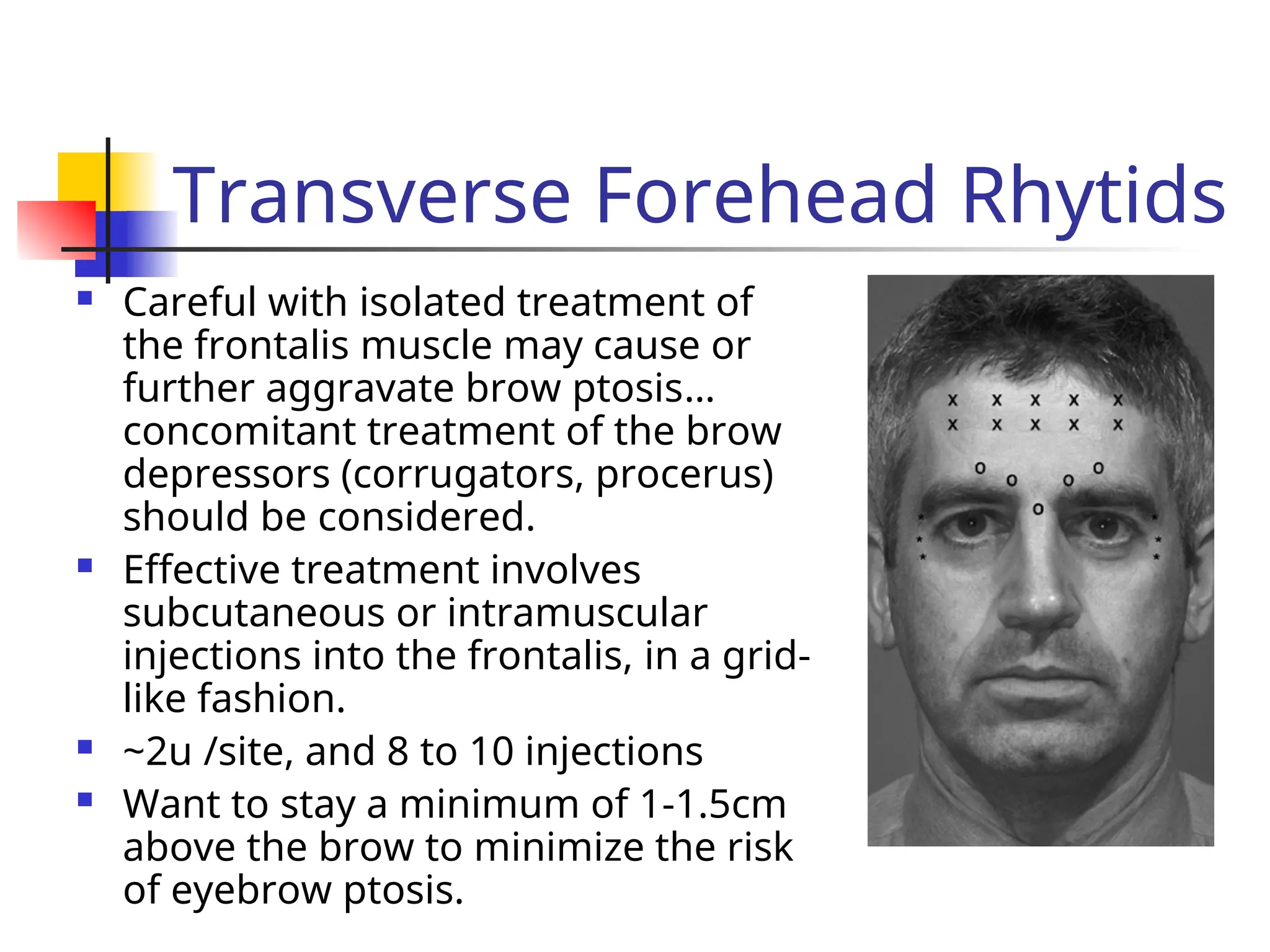
Careful with isolated treatment of
the frontalis muscle may cause or
further aggravate brow ptosis…
concomitant treatment of the brow
depressors (corrugators, procerus)
should be considered.
Effective treatment involves
subcutaneous or intramuscular
injections into the frontalis, in a grid-
like fashion.
~2u /site, and 8 to 10 injections
Want to stay a minimum of 1-1.5cm
above the brow to minimize the risk
of eyebrow ptosis.
12.
Lateral Periorbital Rhytids
“Crow’sFeet”
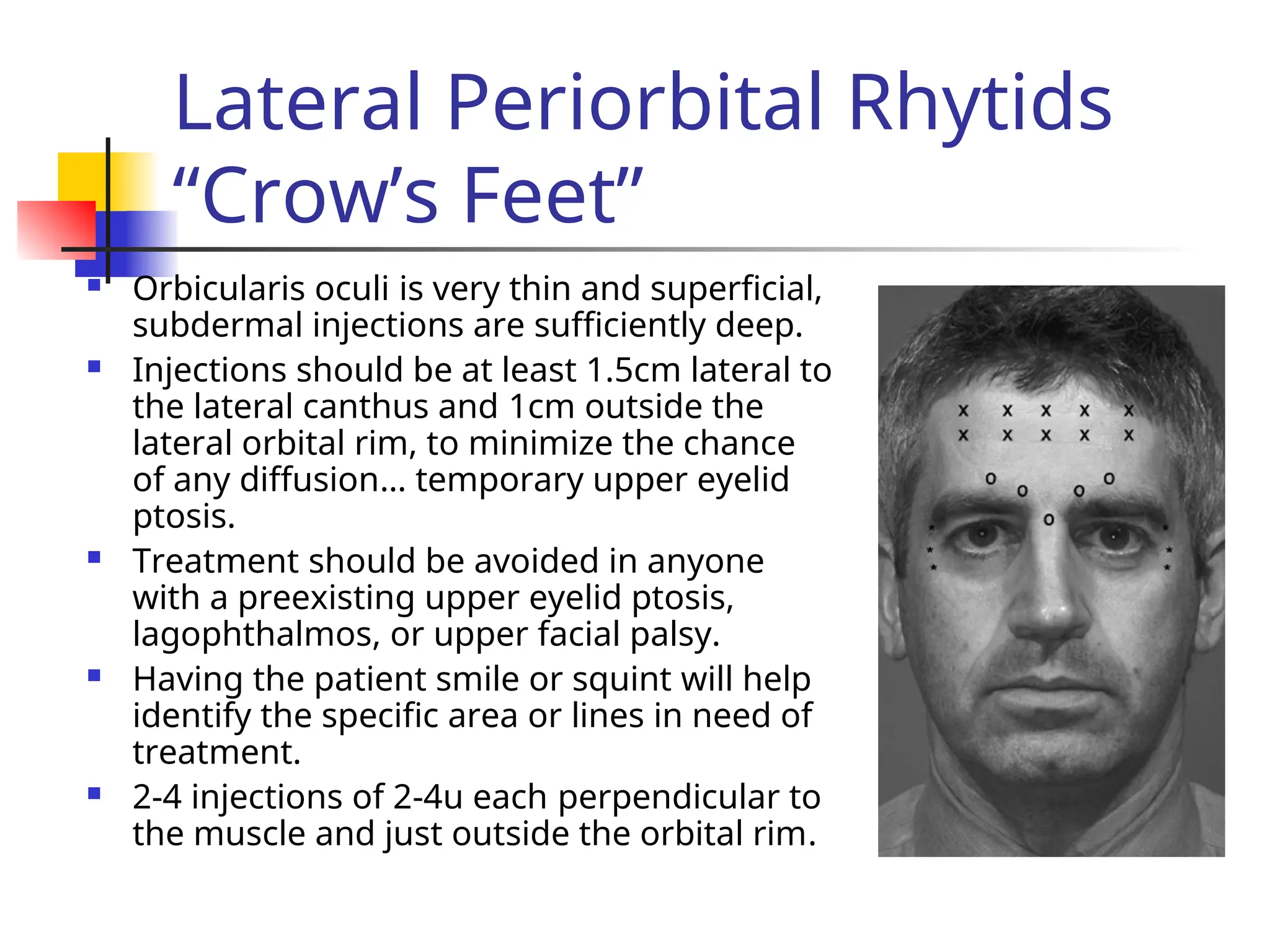
Orbicularis oculi is very thin and superficial,
subdermal injections are sufficiently deep.
Injections should be at least 1.5cm lateral to
the lateral canthus and 1cm outside the
lateral orbital rim, to minimize the chance
of any diffusion… temporary upper eyelid
ptosis.
Treatment should be avoided in anyone
with a preexisting upper eyelid ptosis,
lagophthalmos, or upper facial palsy.
Having the patient smile or squint will help
identify the specific area or lines in need of
treatment.
2-4 injections of 2-4u each perpendicular to
the muscle and just outside the orbital rim.
13.
Chemical Browlift
Browposition is the result of an equilibrium reached between
elevators and the depressors
selective weakening of the brow depressors either medially or
laterally, may result in a modest brow lift.
For elevation of the medial brow, treatment of the corrugators
and procerus, as well as the depressor supercilii is required. The
latter muscle is treated with an injection of 2-4u just below and
just lateral to the medial head of the brow… remain outside the
orbital rim to avoid unwanted diffusion into adjacent muscles.
Elevation of the lateral brow requires a subdermal injection of
the orbicularis oculi muscle just below the eyebrow lateral to the
high point of the brow, once again remaining outside the orbital
rim.
1-3 injections for a total of 4-10u
14.
Platysma Banding
Havingthe patient contract the muscle will to
show the platysmal bands,
Band is grasped and injected with 5u each at
multiple sites 1-1.5cm apart, from below the
jawline to the lower neck.
Each band will receive a total of 15 units, with
treatment of 2 to 4 bands, totaling 30 to 60 units.
Avoid excessive doses and injecting into the
muscle but not deep, to avoid dysphagia and
neck weakness.
15.
Vertical Lip Rhytids
Very superficial (subdermal), very low doses injected
into the upper lip can help soften vertical upper lip
lines.
This treatment may be an alternative to perioral
chemical peels or laser resurfacing, and can be used
alone or in combination with injectable fillers.
Professional public speakers and wind instrument
musicians may not be ideal candidates for this
treatment.
4 evenly spaced injections of 1-2u given across the
upper lip at or immediately above the vermilion border.
Some degree of lip eversion can be expected
16.
Complications
Good safetyprofile
since the effect of Botox is a temporary one, so too
are the complications.
There have been no deaths reported or adverse long-
term effects from cosmetic use
Most complications are site-specific and best avoided
with technical expertise… lowest dose, small volume,
correct depth, stay outside orbital rim etc.
Medications that might potentiate the activity of Botox
include aminoglycosides, cyclosporins, neuromuscular
blockers, calcium channel blockers, quinidine,
magnesium sulfate, and D-penicillamine
17.
Complications
General sequellaeof Botox injections include pain,
erythema and bruising at the injection site,
headache, flu-like symptoms, malaise, and fatigue.
The most significant complication of glabellar or
lateral periorbital injections is upper eyelid ptosis
from migration of Botox
Usually resolves within 2 to 6 weeks.
Ptosis can be treated with alpha-adrenergic
ophthalmic drops, such as Iopidine 0.5% or
Phenylephrine 2.5%, which stimulate Mueller's
muscle to help elevate the eyelid margin
18.
Complications
Resistance toBotox may result from the
formation of neutralizing antibodies.
This is generally associated with repeated
use of high doses (>300u) and is
uncommon with the lower doses used for
cosmetic applications
Patient dissatisfaction may result from
either over-treatment or under-treatment,
and unmet or unrealistic expectations.
19.
Soft-Tissue Augmentation
Hasbeen used for >100 yrs, injecting Pts fat
into defects (Neuber)
In early part of the 1900s, paraffin injection
became popular… granulomatous-type
reactions occurred resulting in paraffinomas.
In the 1940s to 1950s, silicone was introduced…
long-term studies with this showed it resulted
in granulomatous reactions and scarring,
In the 1970s, Stanford researchers developed
bovine collagen, which is still in use today
20.
Xenografts-Bovine Collagen
longesttrack record, gold standard to which other
fillers are compared.
3 types are available: Zyderm I, Zyderm II, and Zyplast
Zyderm is recommended for superficial, mild-to-
moderate wrinkles such as the glabellar creases,
periorbital crow's feet, and perioral rhytids, and the
material should be place in the upper dermis.
Because of early resoprtion with this material,
overcorrection is recommended.
Zyplast is injected into the deeper reticular dermis,
and because it is more resistant to resorption,
overcorrection is not needed
21.
Bovine Collagen
significantdisadvantage of bovine collagen is the
risk of a hypersensitivity reaction displayed as
induration, erythema, pruritus, and tenderness at
the injection site.
Skin testing for allergic sensitivity is therefore
required before definitive use.
~3-4% of patients undergoing skin testing will
display a hypersensitivity reaction
Bovine collagen can result in tissue necrosis, foreign
body reactions, and infrequent systemic reactions,
such as headache, nausea, and arthralgias.
22.
Xenografts-Hyaluronic Acid
Products (Hylaform,Restylane)
Hyaluronic acid is a macromolecule composed of
repeating disaccharide units in the family of
glycosaminoglycans.
This is one of the major components of the
extracellular matrix in the dermis.
It has the ability to bind 1,000x its volume in water,
Hyaluronic acid is unique in that it is identical in all
species… not antigenic across
The injected product is degraded locally and then
metabolized by the liver into carbon dioxide and
water.
23.
Hylaform
Hylaform isa purified animal product
made from rooster combs.
An extremely pure gel.
There have been few reports of any
local or systemic reactions
60% of rhytids showed some degree of
correction 18 months after injection
24.
Restylane
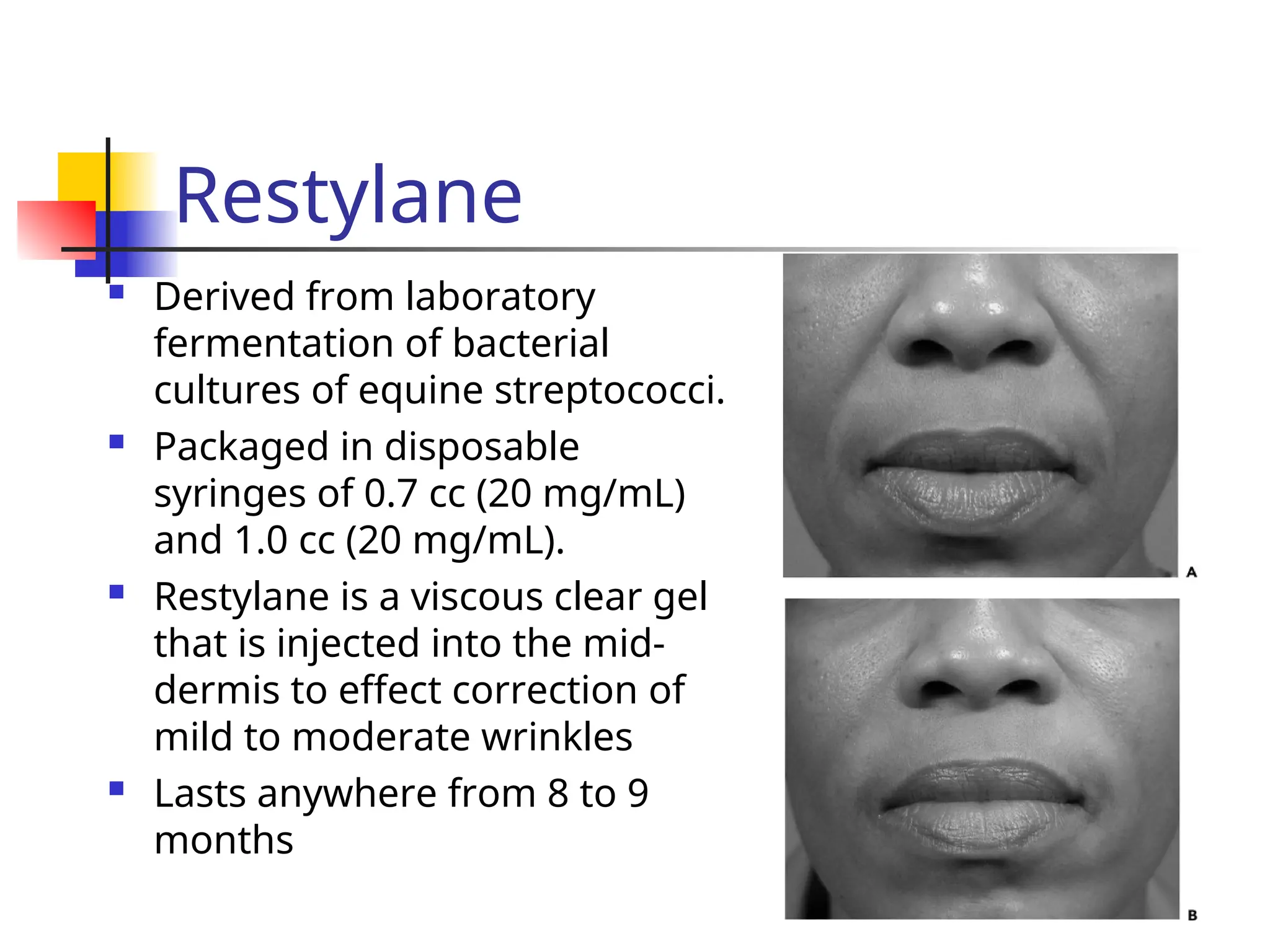
Derived fromlaboratory
fermentation of bacterial
cultures of equine streptococci.
Packaged in disposable
syringes of 0.7 cc (20 mg/mL)
and 1.0 cc (20 mg/mL).
Restylane is a viscous clear gel
that is injected into the mid-
dermis to effect correction of
mild to moderate wrinkles
Lasts anywhere from 8 to 9
months
25.
Autografts-Autologous Fat
longesthistory of use
there is no universally accepted method for the
harvesting, processing, and reinjection of
autologous fat
often results are not reproducible.
The advantage of fat transplantation is the large
amounts available in the human body, and
because it is autologous.
Donor site morbidity
Fat grafting has the disadvantage of having an
unpredictable resorption rate (30-60% resorption)
26.
Autografts-Isolagen
A wayto inject patients with their own fibroblasts,
Start with a 3-mm punch of skin harvested from
the patient's postauricular area.
The specimen is sent to the Isolagen laboratories,
where it is cultured in vitro, together with growth
factors, to produce an amount of living fibroblasts.
The syringe with the fibroblasts is then returned to
the doctor's office for injection into the patient the
following day.
Several treatments are required $$$, impractical?
Initial results have been encouraging.
27.
Homografts-CosmoDerm
and CosmoPlast
Humancollagen
derived from bioengineered human fibroblasts,
no pretesting is required
CosmoDerm is indicated for superficial lines and
wrinkles,
CosmoPlast (cross-linked with glutaraldehyde) is
better able to treat deeper grooves and scars. T
hese products are longer lasting than bovine
collagen, on average, they will last for 3-6 months.
28.
Homografts-Alloderm
AlloDerm isan acellular, freeze-dried dermal graft
processed from human cadaver dermis.
It is available in sheets as AlloDerm and in an
injectable form Cymetra (micronized AlloDerm).
The freeze-drying process removes all the cells,
leaving collagen IV and VII and elastin.
It integrates rapidly into the surrounding tissue,
showing neovascularization by the
No skin testing is required
No long-term studies are yet available, supposed
to be long-lasting
Synthetics-Artecol
It iscomposed of 30 to 40 micron spheres of polymethyl
methacrylate (PMMA) suspended in 3.5 % bovine collagen.
Theoretically, as the collagen resorbs over a period of
months, the PMMA spheres become encapsulated by
fibrous tissue, ensuring a constant augmentation
This material needs to be injected into the subdermis;
otherwise, a persistent painful nodule may persist.
Skin testing is required
Some studies showed satisfactory results others reported
multiple foreign body granulamatous reactions, and poor
results,
Not FDA approved
31.
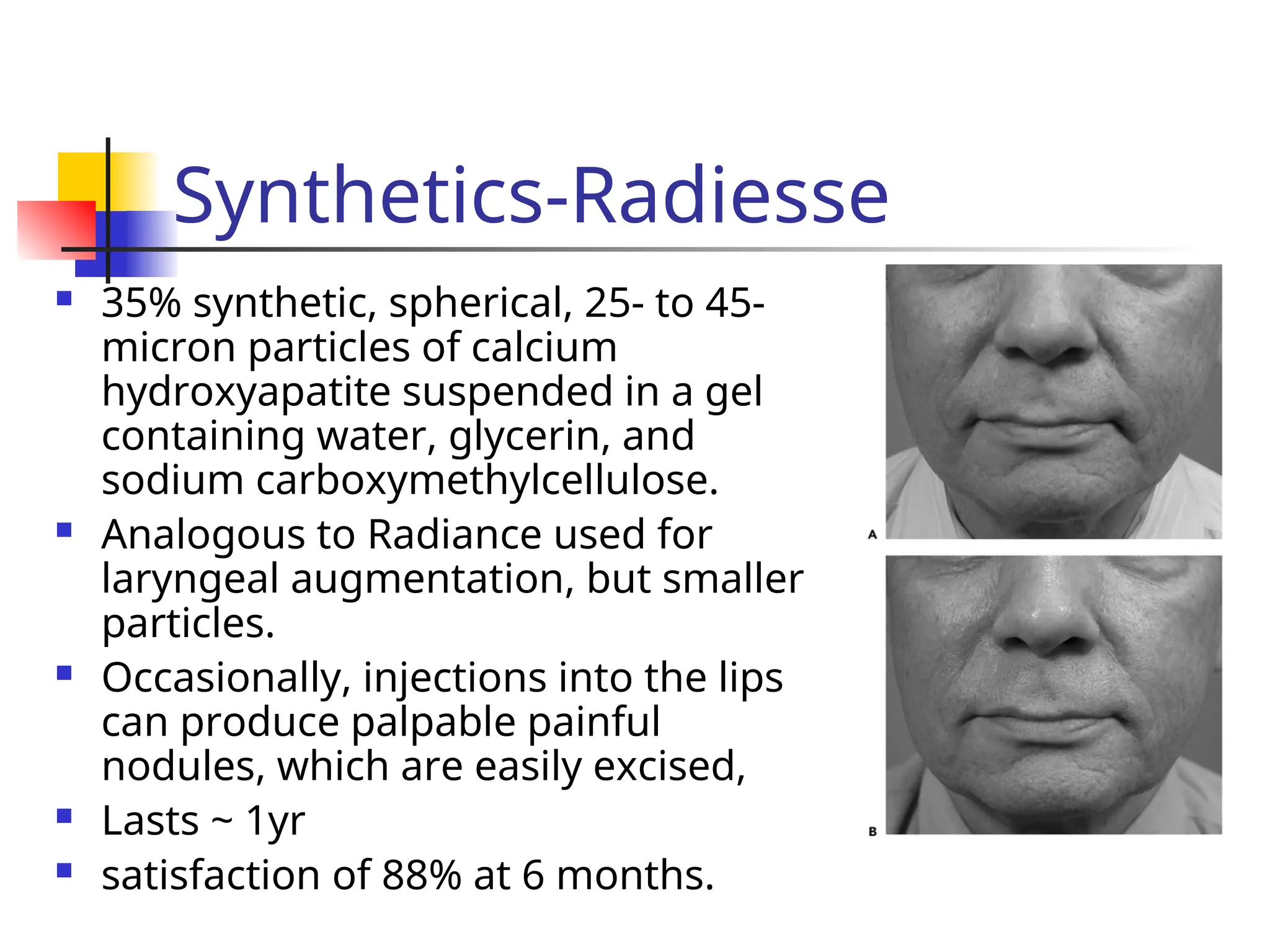
Synthetics-Radiesse
35% synthetic,spherical, 25- to 45-
micron particles of calcium
hydroxyapatite suspended in a gel
containing water, glycerin, and
sodium carboxymethylcellulose.
Analogous to Radiance used for
laryngeal augmentation, but smaller
particles.
Occasionally, injections into the lips
can produce palpable painful
nodules, which are easily excised,
Lasts ~ 1yr
satisfaction of 88% at 6 months.







![Treatment of periorbital_rhytids_with_botox[1]](https://cdn.slidesharecdn.com/ss_thumbnails/treatmentofperiorbitalrhytidswithbotox1-130422140956-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































