Download to read offline



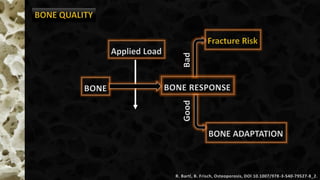



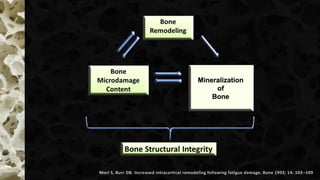

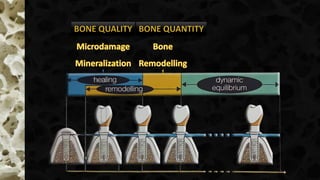

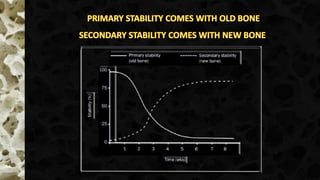
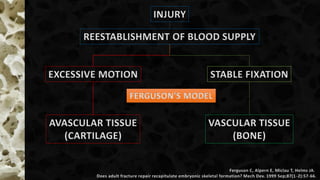


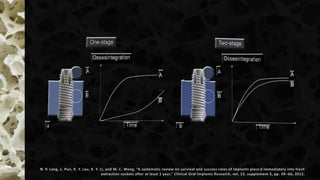
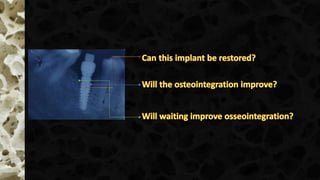

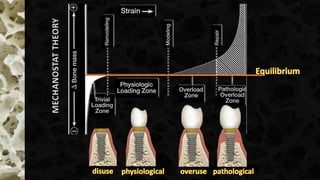

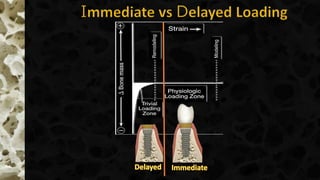



This document discusses bone biology and physiology related to dental implants. It addresses questions about waiting periods for implants in the maxilla and mandible, the benefits of augmentation versus simultaneous implantation, and differences between immediate and delayed loading. It also covers topics like bone quality determinants, osseointegration factors, bone response to injury, remodeling processes, and theories related to mechanotransduction and healing.





















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
