Download to read offline










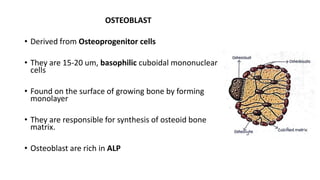


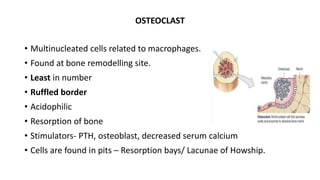




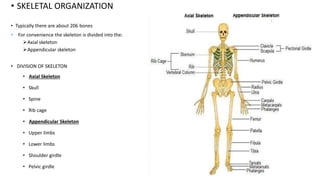












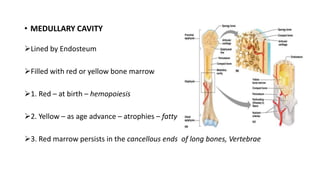













































This document provides an overview of bone anatomy, histology, and blood supply. It discusses that bone is a dynamic connective tissue composed of an organic matrix and inorganic minerals. It describes the cellular components of bone including osteoblasts, osteoclasts, and osteocytes which are responsible for bone formation, resorption, and remodeling. The document outlines the classification of bones and explains the structure of long bones including the diaphysis, metaphysis, and epiphysis. It provides details on cortical and cancellous bone, woven and lamellar bone, and the microstructure of compact and spongy bone.


















































































