Downloaded 315 times


![SAFETY
• The performed animal experimental investigations
indicated for bisoprolol no unexpected or serious side-
effects.
• Even at high doses [30 and 100mg/ kg, single oral
administration(rats)], the sedative effects ascribed to
b-blockers are less marked with bisoprolol than, for
instance, with propranolol .](https://image.slidesharecdn.com/asadullahans-130402213511-phpapp02/85/Bisoprolol-21-320.jpg)
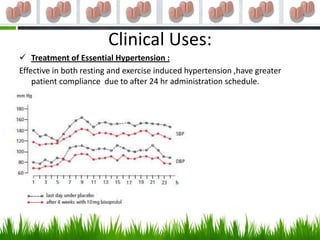



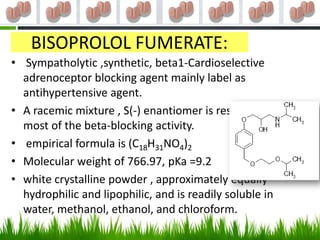
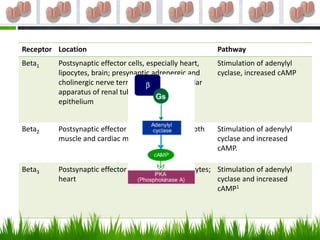
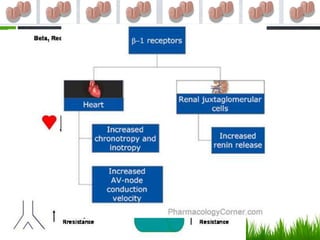
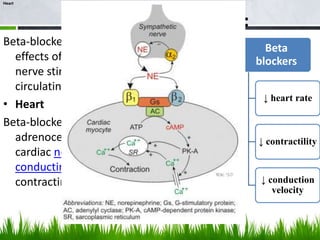
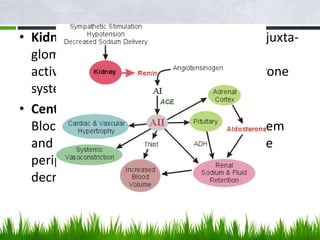
This document discusses bisoprolol, a beta-1 selective adrenoceptor blocking agent used to treat hypertension and angina. It provides details on bisoprolol's history, pharmacological properties, therapeutic indications, contraindications, adverse reactions, and toxicological studies. Bisoprolol is a highly selective beta-1 blocker that is well-absorbed orally and has a half-life of 10-12 hours. It is used to treat hypertension, angina, and heart failure by reducing heart rate and contractility. Adverse effects include fatigue, dizziness, and bronchospasm. Toxicology studies found it to be non-cytotoxic, non-mutagenic, and























































































