Bartter syndrome is a genetic disorder characterized by hypokalemia, hypochloremia, metabolic alkalosis, and hypercalciuria. It results from defects in sodium, chloride, and potassium transporters in the ascending loop of Henle. There are four main types based on the underlying molecular defects. The neonatal form presents in newborns with severe salt wasting, dehydration, and hypotension. Classic Bartter syndrome presents in older infants and children with muscle cramps, weakness, and growth failure due to chronic hypokalemia. Treatment involves potassium and sodium supplementation and potassium-sparing diuretics. With adequate treatment, long-term prognosis is generally good, though some may have chronic complications
Porphyrias are difficult to diagnose . Here it is comprehensively explained to aid making diagnosis of porphyrias easier for the benefit of medical students and practitioners.
Porphyrias are difficult to diagnose . Here it is comprehensively explained to aid making diagnosis of porphyrias easier for the benefit of medical students and practitioners.
refsum disease its a genetical disorder which is autosomal recessive phytanoyl-CoA-hydroxylase is the enzyme location of this enzyme is chromosome 10p13
refsum disease its a genetical disorder which is autosomal recessive phytanoyl-CoA-hydroxylase is the enzyme location of this enzyme is chromosome 10p13
One of lectures presented in our Port said fifth neonatology conference 23-24 October 2014, presented by prof Olfat Fawzy, M.D, M.Sc.,Professor of Endocrinology Al Azhar university
Obstructive jaundice also called surgical jaundice defined as jaundice which can be treated by any surgical procedure or by any intervention. Surgical and medical gastroenterologists play great role in treating such patients , however interventional radiologists also have great role in treating such patients.
The Art Pastor's Guide to Sabbath | Steve ThomasonSteve Thomason
What is the purpose of the Sabbath Law in the Torah. It is interesting to compare how the context of the law shifts from Exodus to Deuteronomy. Who gets to rest, and why?
Instructions for Submissions thorugh G- Classroom.pptxJheel Barad
This presentation provides a briefing on how to upload submissions and documents in Google Classroom. It was prepared as part of an orientation for new Sainik School in-service teacher trainees. As a training officer, my goal is to ensure that you are comfortable and proficient with this essential tool for managing assignments and fostering student engagement.
2024.06.01 Introducing a competency framework for languag learning materials ...Sandy Millin
http://sandymillin.wordpress.com/iateflwebinar2024
Published classroom materials form the basis of syllabuses, drive teacher professional development, and have a potentially huge influence on learners, teachers and education systems. All teachers also create their own materials, whether a few sentences on a blackboard, a highly-structured fully-realised online course, or anything in between. Despite this, the knowledge and skills needed to create effective language learning materials are rarely part of teacher training, and are mostly learnt by trial and error.
Knowledge and skills frameworks, generally called competency frameworks, for ELT teachers, trainers and managers have existed for a few years now. However, until I created one for my MA dissertation, there wasn’t one drawing together what we need to know and do to be able to effectively produce language learning materials.
This webinar will introduce you to my framework, highlighting the key competencies I identified from my research. It will also show how anybody involved in language teaching (any language, not just English!), teacher training, managing schools or developing language learning materials can benefit from using the framework.
Welcome to TechSoup New Member Orientation and Q&A (May 2024).pdfTechSoup
In this webinar you will learn how your organization can access TechSoup's wide variety of product discount and donation programs. From hardware to software, we'll give you a tour of the tools available to help your nonprofit with productivity, collaboration, financial management, donor tracking, security, and more.
Model Attribute Check Company Auto PropertyCeline George
In Odoo, the multi-company feature allows you to manage multiple companies within a single Odoo database instance. Each company can have its own configurations while still sharing common resources such as products, customers, and suppliers.
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
How to Make a Field invisible in Odoo 17Celine George
It is possible to hide or invisible some fields in odoo. Commonly using “invisible” attribute in the field definition to invisible the fields. This slide will show how to make a field invisible in odoo 17.
Operation “Blue Star” is the only event in the history of Independent India where the state went into war with its own people. Even after about 40 years it is not clear if it was culmination of states anger over people of the region, a political game of power or start of dictatorial chapter in the democratic setup.
The people of Punjab felt alienated from main stream due to denial of their just demands during a long democratic struggle since independence. As it happen all over the word, it led to militant struggle with great loss of lives of military, police and civilian personnel. Killing of Indira Gandhi and massacre of innocent Sikhs in Delhi and other India cities was also associated with this movement.
5. Bartter syndrome
• It is a group of disorder characterized by hypokalemic, hypochloremic,
metabolic alkalosis with hypercalciuria and salt wasting .
• First reported by Bartter in 1962
• AR
• Hyperreninemia,hyperaldosteronism also present
• Blood pressure remains normal
• Urine levels of sodium,chloride and potassium are increased
• Two types : neonatal bartter– before or immediately after birth
• classical bartter --- occur in neonates or infants aged 2 yrs or
• younger
6. Pathophysiology
• Resembles those seen with chronic use of loop diuretics
• Reflect a defect in Na,Cl,K transport in ascending loop of henle
loss of
Na,cl
Volume
contraction
Stimulate
RAAS
Aldosterone increase Na
uptake & K excretion &
exacerbate
hypokalemia,stimulate H+
secretion distally
hypokalemia stimulate PG
synthesis
7. • 4 types based on the underlying molecular defects in the following loop of
henle transporters ,
• Na/K/2Cl transporter (NKCC2,the site of action of furosemide )
• The luminal potassium channel(ROMK)
• Combined chloride channel (CLC-Ka,CLC-Kb)
• Subunit of chloride channels (barttin)--- these cause neonatal barter
syndrome
• Isolated defects in genes that produce a specific basolateral chloride channel
(ClC-Kb ) cause classic barters syndrome
8. • Type 1,2,4 are neonatal forms , i.e, antenatal barter ,also known as
hyperprostagalndin E syndrome
• Type 3 – classical barter syndrome
9.
10. Clinical features of barters syndrome
• In neonatal bartter
• Generally born preterm
• Marked intrauterine polyuria—polyhydramnios
• Polyuria upto 12-50 ml/kg/hr continues postnatally and cause severe
dehydration
• Dysmorphic features include
• Trangular facies,protruding ears ,large eyes with strabismus ,drooping
mouth
11.
12. • Older children have muscle cramps,weakness,secondary to chronic
hypokalemia ,polyuria,polydipsia ,growth failure,chronic
constipation,dizziness
• Bp usually normal,but patients with antenatal form can have severe salt
wasting – dehydration and hypotension
• Renal function typically normal
• Marked hypercalciuria with nephrocalcinosis is consistent with neonatal
form and rare in classic type
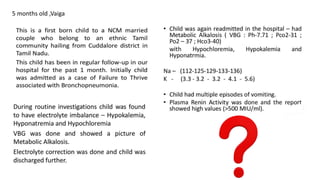
13. Diagnosis
• Based on clinical presentation and lab findings
• In neonate / infant – severe hypokalemia(usually <2.5mmol/L)
,hyponatremia,Metabolic alkalosis,hyperaldosteronism, increased
renin,hyperuricemia ,hypercalciuria,nephrocalcinosis will be present often
• Hypomagnesemia present in minority only ( but more common in
gittelman)
• Differential diagnosis
• diuretic abuse
• Chronic vomiting
• Cystic fibrosis urinary Cl is low in these but increased in bartters
14. Treatment
• Primary aim to correct hypokalemia,volume deficit,maintain nutritional
status
• KCl given 1-3 mEq /kg/day
• Additionally K sparing diuretics spironolactone 10-15 mg/kg/day or
triamterene 10mg/kg/day may be used
• Most effective drugs are PG synthetase inhibitors ,mainly indomethacin 2-
4 mg/kg/day,but look for s/e nausea,vomiting,abdominal pain ,peptic
ulcer ,renal,hepatic toxicity
• Infants and young children require high Na diet,and at times Na
supplementation .
• If needed supplement Mg also .
15. prognosis
• Long term prognosis with adequate treatment is generally good
• In a minority, chronic hypokalemia,nephrocalcinosis,can occur
• Chronic indomethacin therapy can lead to chronic interstitial nephritis
and chronic renal failure
16. GITTELMAN SYNDROME
• A/k/a bartter syndrome variant
• AR
• Pathophysiology
• Due to defective functioning of thiazide sensitive NaCl co transporter
(NCCT)of distal convoluted tubule due to inactivating mutations in the gene
SLC12A3,locus 16q13
• Hypokalemic , hypochloremic metabolic alkalosis with distinct features of
hypocalciuria and hypomagnesemia
• Biochemical features resemble chronic use of thiazide diuretics
17. Clinical features
• Present in late childhood or early adulthood
• Symptoms similar to older children with bartter
• Recurrent muscle cramps,spasms,due to low serum Mg levels
• Nocturia,polyuria,occasional hypotension
• Biochemically : hypokalemia
• metabolic alkalosis
• Hypomagnesemia
• Urine Ca level very low
Urine Mg level low
Renin& aldosterone levels normal
Prostaglandin E not elevated
Growth failure is less prominent compared to bartters
18. Diagnosis
• When an adolescent or adult presenting with hypokalemia , hypochloremia,
metabolic alkalosis, hypomagnesemia, hypocalciuria
• Treatment
• K & Mg supplementation
• Na supplementation or PG inhibitors are not needed
• Prognosis
• Excellent long term outcome with preserved renal function
19.
20. Other inherited tubular transport abnormalities
• Cystinuria
• AR
• Characterised by recurrent stool formation
• Due to defective high affinity transporter for L cystine and dibasic
aminoacids present in proximal tubule
• Dent disease
• X linked proximal tubulopathy with low molecular weight
proteinuria,hypercalciuria,and other features of Fanconi syndrome like
glycosuria,aminoaciduria,phosphaturia
21. • Gordon syndrome (familial hyperkalemic hypertension)
• Occur in DCT
• Due to gain of function mutation of WNK 1 and loss of function mutation of
WNK 4 ,both serine threonine kinases ,lead to excessive NCCT mediated
salt reabsorption
• Clinical picture is of pseudohypoaldosteronism type 2 i.e,
• Volume expansion with HTN
• Hyperkalemia
• Hyperchloremic metabolic acidosis
• Hypercalciuria
• Treatment : thiazide diuretics
22. Liddle syndrome
• Occur in collecting duct
• Gain of function mutation of gene encoding ENaC
• Clinical feature : HTN
• They have constitutive Na uptake in collecting duct with hypokalemia &
supressed aldosterone
• Treatment: amiloride like potassium sparing diuretics
•Pseudohypoaldosteronism
• Due to loss of function mutation of ENaC
• Severe Na wasting ,hyperkalemia &distal RTA (type1V)
23. Renal hypouricemia
• Defect in SLC22A12 gene
• Clinical features: low serum uric acid levels
• Exercise induced acute renal failure ( loin pain,nausea,vomiting after
exercise)
• Elevated urine uric acid levels
• Treatment : of acute renal failure and reducing the intensity of exercise