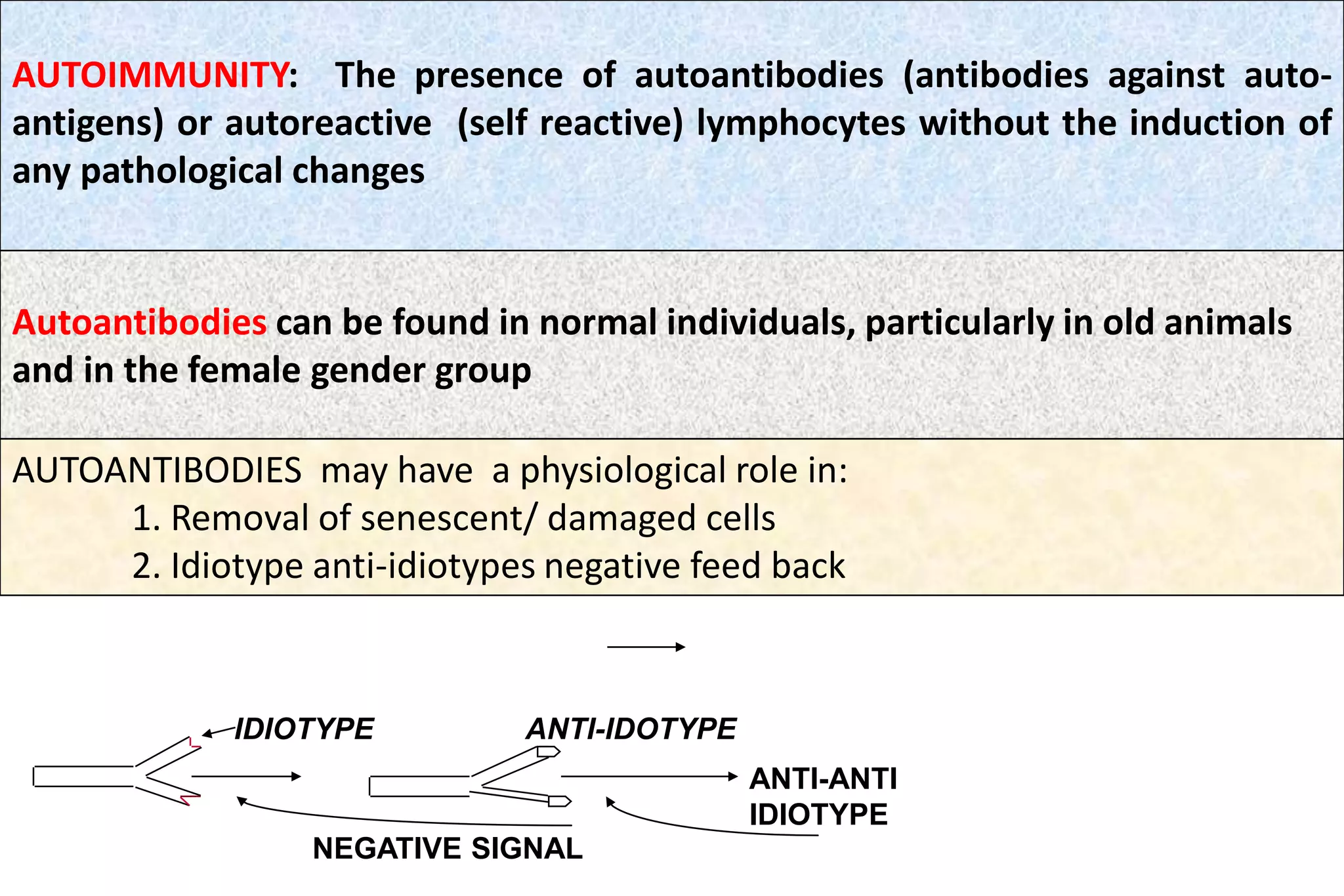
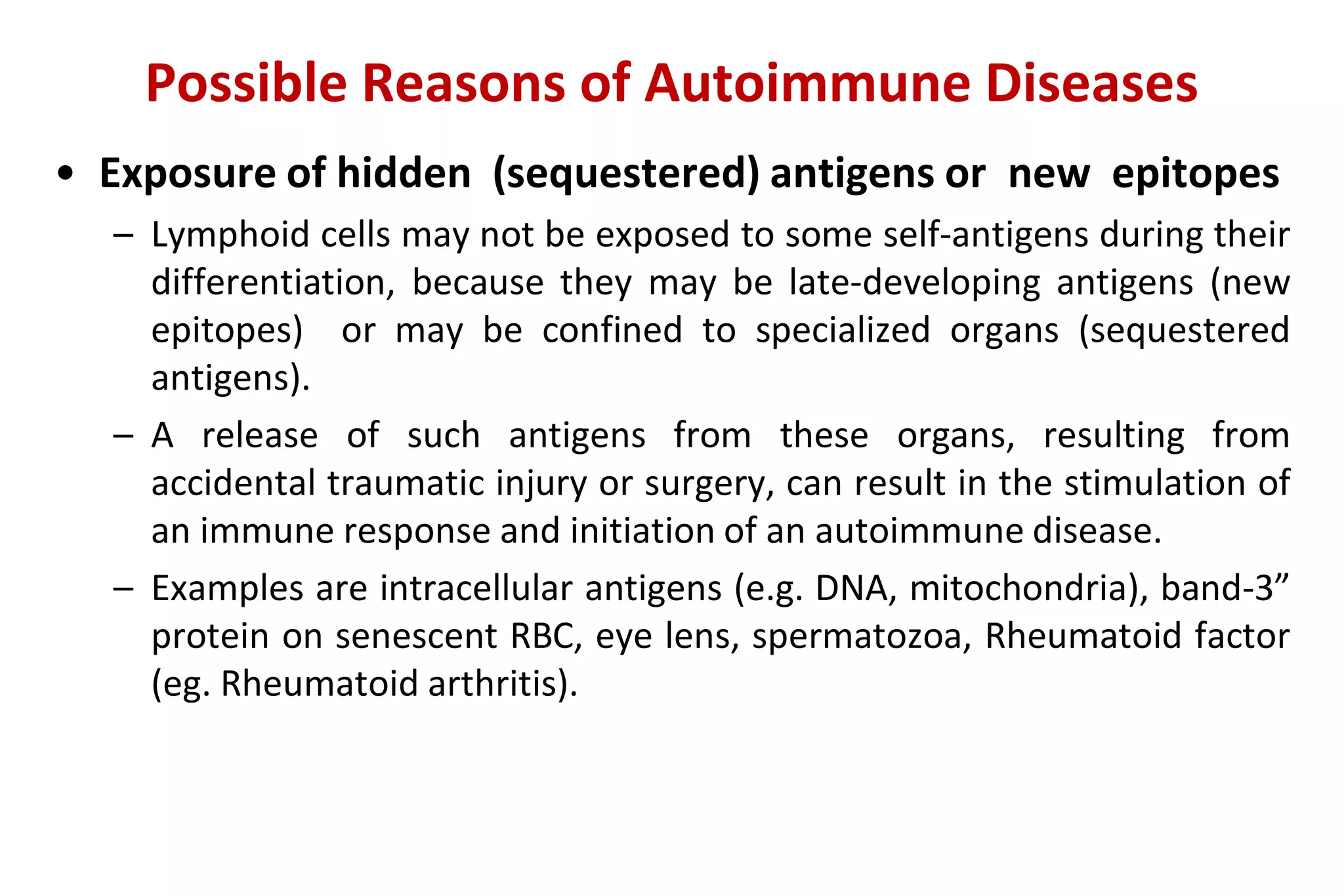
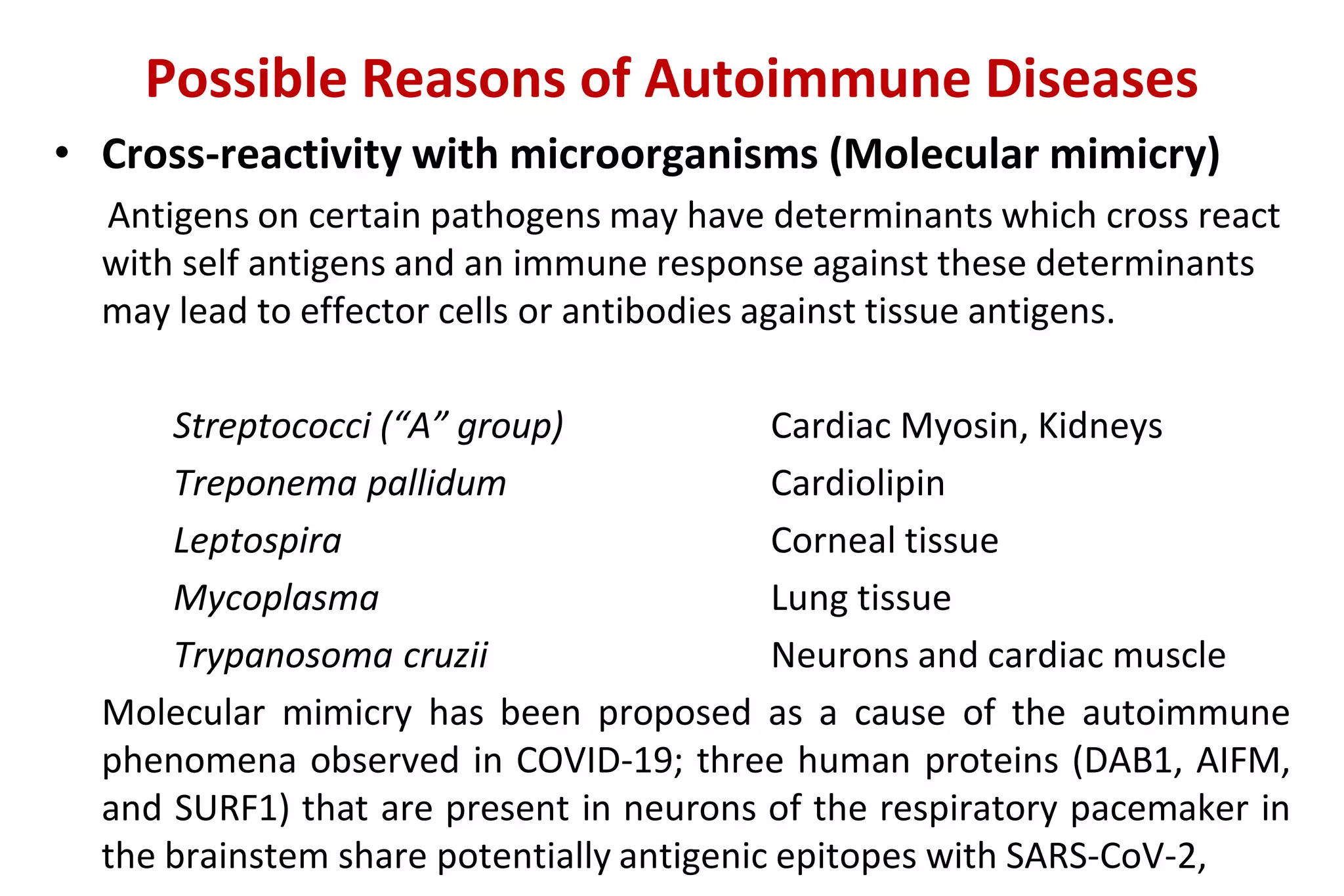
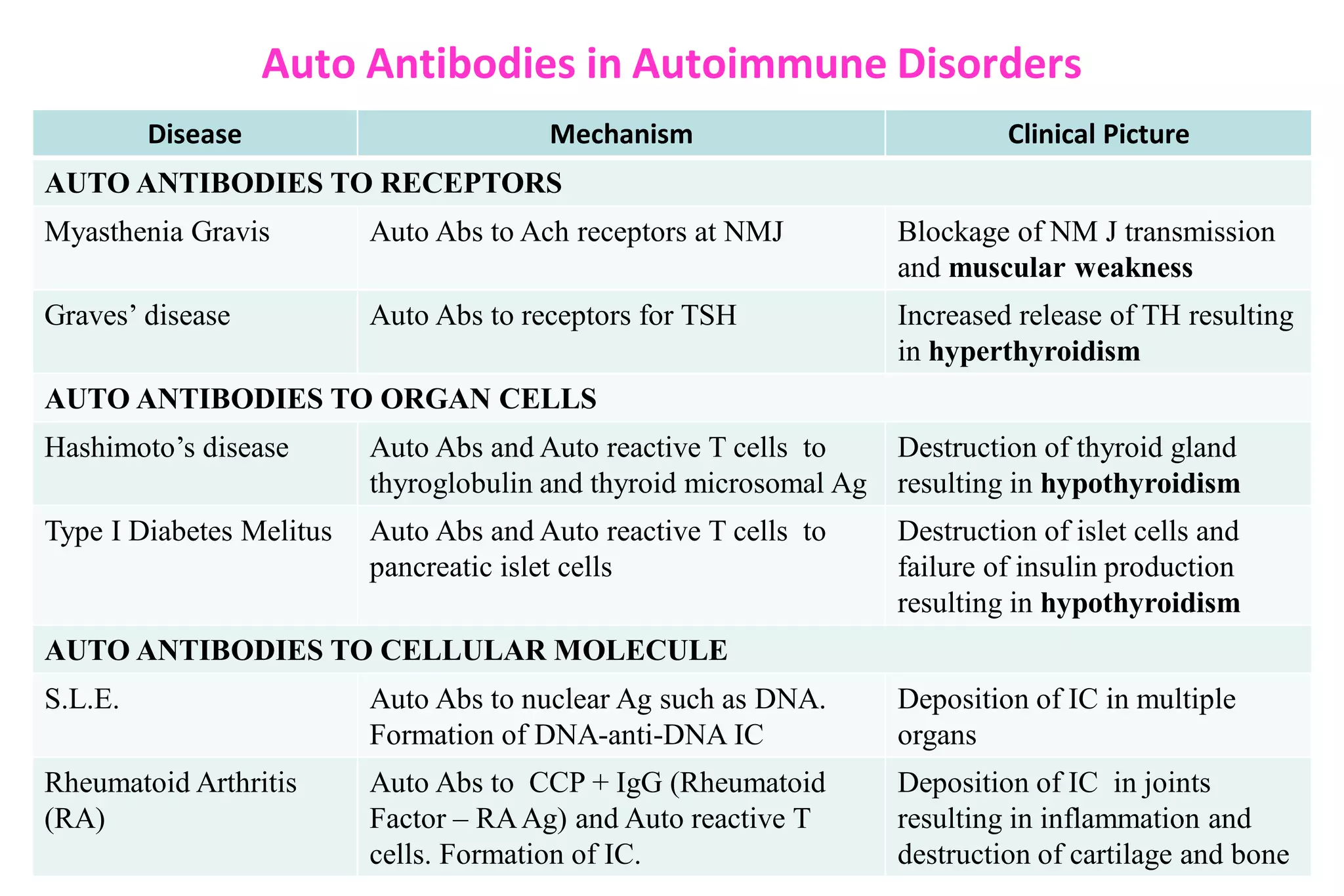
Autoimmunity results from a failure of self-tolerance mechanisms in the immune system. This allows autoreactive lymphocytes and autoantibodies that target self-antigens to develop. A combination of genetic, environmental, and immunological factors contribute to autoimmune diseases. Tissue damage in these diseases can occur through various mechanisms, including cytotoxic antibodies, immune complexes, and T-cell mediated responses, leading to pathological changes in organs and tissues. Common autoimmune diseases involve autoreactivity against receptors, organ-specific cells, or cellular molecules like DNA and rheumatoid factor.




![(Bellanti JA (Ed). Immunology IV: Clinical Applications in Health and Disease. I Care Press, Bethesda, MD, 2012].)
The Three Etiopathogenic Factors Involved In Autoimmune
Diseases.](https://image.slidesharecdn.com/autoimmunity-and-autoimmune-disorders-220914174020-bbbeac07/75/Autoimmunity-and-Autoimmune-disorders-pdf-8-2048.jpg)




![Mechanisms of issue damage
• Mechanisms involved in tissue damage are very complex.
• In a number of autoimmune diseases more than one mechanism are involved.
• IgE autoantibodies ( Type I ): Rare. A possible example: “Milk allergy” in Jersey
cattle; IgE autoantibody response to α-casein.
• Cytotoxic (Type II ):
Autoantibodies to cell surface, e.g.
RBC........................autoimmune hemolytic anemia
Thrombocytes....... autoimmune thrombocytopenia
• Immunecomplex (Type III):
Autoantibodies (Ab) + Antigen (Ag) [ Ab-Ag ] Immunecomplex, e.g. SLE, RA
• T-Cell Mediated Damage (Type IV):
T cells are primarily involved in tissue damage, e.g. autoimmune thyroiditis,
ulcerative colitis, Insulin-dependent Juvenile-onset Diabetes, autoimmune
encephalitis](https://image.slidesharecdn.com/autoimmunity-and-autoimmune-disorders-220914174020-bbbeac07/75/Autoimmunity-and-Autoimmune-disorders-pdf-16-2048.jpg)








































![Small pox virus [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/smallpoxvirusautosaved-211115161222-thumbnail.jpg?width=640&height=640&fit=bounds)











































