Expectations
• Purpose
Understand pathogenicityin the immune
system
• Objectives
Explain the immunopathology
Define major types of immunopathologies
Apply knowledge in tissue immunology and
immunoprophylaxis
3.
• What we’llbe doing
Lectures/discussions
Some practicals
Group discussions and presentation of articles
• Course Assessment
CATs – 30%
Exam – 70%
4.
Hypersensitivity Reactions
• Reactionscaused by immune responses
• based on the observation that an individual who has
been exposed to an antigen exhibits a detectable
reaction, or is “sensitive” to subsequent encounters
with that antigen.
• As a result of responses that are inadequately
controlled or inappropriately targeted to host tissues.
• Can be looked at as hypersensitivity disorders or
diseases
5.
Causes of hypersensitivitydiseases
• Immune responses may be pathologic due to
several different abnormalities
Autoimmunity
- Reactions against one’s own cells and tissues
- Results in autoimmune diseases
Reactions against microbes
- Excessive reactions
- Unusual persistence of microbes (leads severe
inflammation e.g. in TB)
6.
Reactions against environmentalantigens
- Almost 20% of the population is abnormally
responsive to these substances.
• Hypersensitivity diseases tend to be chronic,
often debilitating, and therapeutic challenges
• Chronic Inflammation is a major component of
the pathology of these disorders and as such
may sometimes be referred to as inflammatory
diseases
Causes of hypersensitivity diseases
7.
Classification of HypersensitivityDisorders
• Commonly classified according to the type of
immune response and the effector mechanism
responsible for cell and tissue injury
Pathogenesis of Autoimmunity
•Autoimmunity results from a failure or breakdown
of mechanisms normally responsible for
maintaining self-tolerance in B cells, T cells, or both.
• The major factors that contribute to the
development of autoimmunity are genetic
susceptibility and environmental triggers, such as
infections
• Autoimmune diseases may be either systemic (e.g.
SLE) or organ specific (e.g. MS)
18.
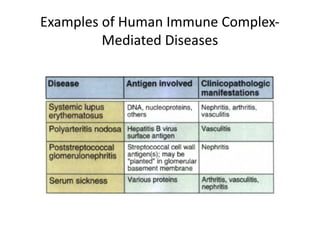
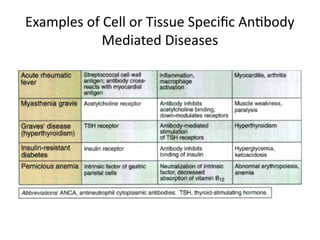
Pathogenesis of Autoimmunity
•Various effector mechanisms are responsible for tissue
injury in different autoimmune diseases. These include
immune complexes, circulating autoantibodies, and
autoreactive T lymphocytes.
• Autoimmune reactions initiated against one self antigen
that injure tissues may result in the release and
alterations of other tissue antigens, activation of
lymphocytes specific for these other antigens, and
exacerbation of the disease. This phenomenon is called
epitope spreading, and it may explain why once an
autoimmune disease has developed, it tends to be
chronic and often progressive.
19.
Role of Infectionsin Autoimmunity
Infections of particular tissues may induce
local innate immune responses that recruit
leukocytes into the tissues and result in the
activation of tissue APCs. This may result in
responses that are not specific for the
infectious pathogen (bystander activation).
20.
Role of Infectionsin Autoimmunity
Infectious microbes may contain antigens that
cross-react with self antigens so immune
responses to the microbes may result in
reactions against self antigens (molecular
mimicry)
21.
Role of Infectionsin Autoimmunity
Microbes may engage Toll-like receptors (TLRs)
on dendritic cells, leading to the production of
lymphocyte-activating cytokines, or on
autoreactive B cells, leading to autoantibody
production. A role of TLR signaling in
autoimmunity has been demonstrated in
mouse models of SLE, but its significance in
human autoimmune diseases is unclear.
22.
Other Factors inAutoimmunity
• Anatomic alterations in tissues, caused by
inflammation, ischemic injury, or trauma, may
lead to the exposure of self antigens that are
normally concealed from the immune system
and therefore may not have induced self
tolerance
• Hormonal influences play a role in some
autoimmune diseases e.g. in SLE
23.
Therapeutic Approaches forAutoimmune
Diseases
• They are similar to those used to prevent graft rejection
• The mainstay is anti-inflammatory drugs, particularly
corticosteroids. Such drugs are aimed at reducing
tissue injury
• Biologic agents that inhibit immune responses and
inflammation have become important treatment
options. E.g. a soluble form of the TNF receptor and
anti-TNF antibodies that bind to and neutralize TNF are
of great benefit in many patients with rheumatoid
arthritis and Crohn’s disease.
24.
Therapeutic Approaches forAutoimmune
Diseases
• Agents that block B7 costimulators are approved for treatment of
rheumatoid arthritis and psoriasis. These antagonists are now in
clinical trials for SLE and other diseases
• In severe cases, immunosuppressive drugs such as cyclosporine
are used to block T cell activation, or anti-proliferative drugs such
as methotrexate are used to reduce the generation and
expansion of lymphocytes
• Plasmapheresis has been used to reduce levels of circulating
antibodies or immune complexes.
• There are ongoing attempts at more specific treatments, such as
inducing tolerance in disease-producing lymphocyte clones, or
inducing regulatory T cells specific for self antigens.