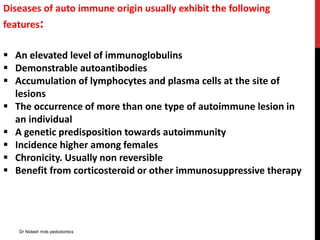
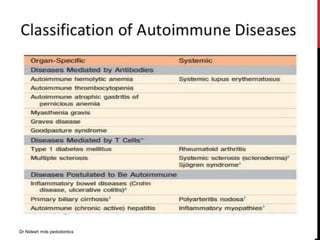
This document provides information on autoimmune disorders, including:
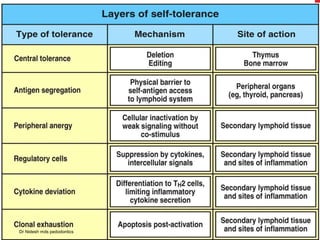
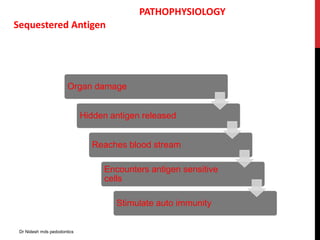
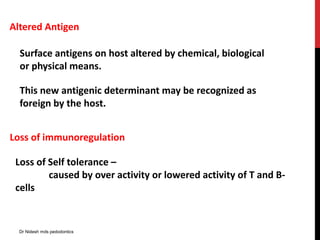
- Causes of autoimmunity include sequestered antigens, altered antigens, loss of immunoregulation, and loss of self-tolerance.
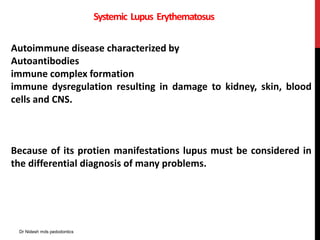
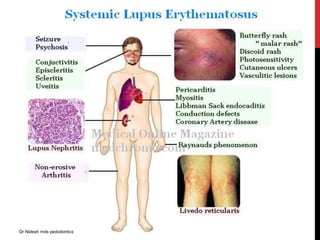
- Common autoimmune diseases discussed include systemic lupus erythematosus and systemic sclerosis.
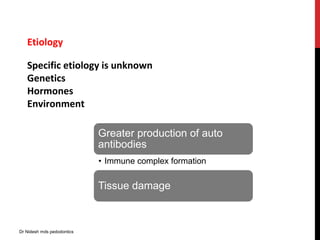
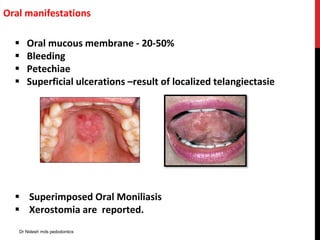
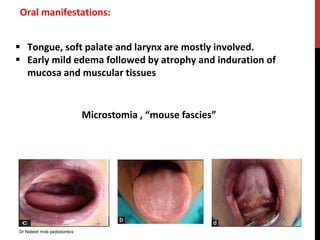
- For systemic lupus erythematosus, clinical manifestations, etiology, pathology, and treatment are summarized. Oral manifestations including bleeding and ulcers are also noted.
- Systemic sclerosis causes fibrosis of the skin, subcutaneous tissue, muscles and internal organs. Its etiology is unclear but involves genetic and environmental factors.



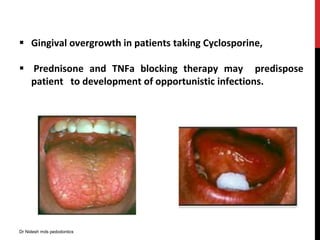
![ A major complicating factor is development of the
pseudolymphoma and malignant lymphoma.
The risk of lymphoma [non hodgkins] in sjogrens syndrome
patients is 6.4 cases for 100 cases.
Dr Nidesh mds pedodontics](https://image.slidesharecdn.com/5thautoimmunedisorderseminar-170204095337/85/auto-immune-disorder-seminar-70-320.jpg)






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






