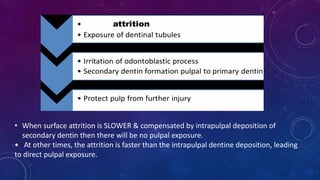
This document discusses dental attrition, which is the mechanical wear of teeth due to functional or parafunctional tooth contact. It classifies attrition into four types based on the amount of tooth structure lost. Proximal and occlusal surface attrition are also described. Factors like bruxism, nail biting and certain occupations can predispose to attrition. Clinical signs include polished facets, flattened cusps, sensitivity and reverse cusping in advanced cases. Management involves patient education, occlusal splints for bruxism, restorations to smooth sharp edges, desensitizing treatments, endodontics or extractions for pulpally involved teeth, and porcelain veneers for incisal wear.



![• In some older patients, the enamel of
the cusp tips or incisal edges is worn off,
resulting in cupped-out areas because
the exposed dentin, softer dentin wears
faster than surrounding enamel. [ reverse
cusping ]
• Advanced attrition – enamel may get
worn away which results in an extrinsic
yellow or brown staining of exposed
dentin from food or tobacco.](https://image.slidesharecdn.com/attritionbydrpc-220914140529-31aeaa33/85/Attrition-by-Dr-PC-pptx-6-320.jpg)