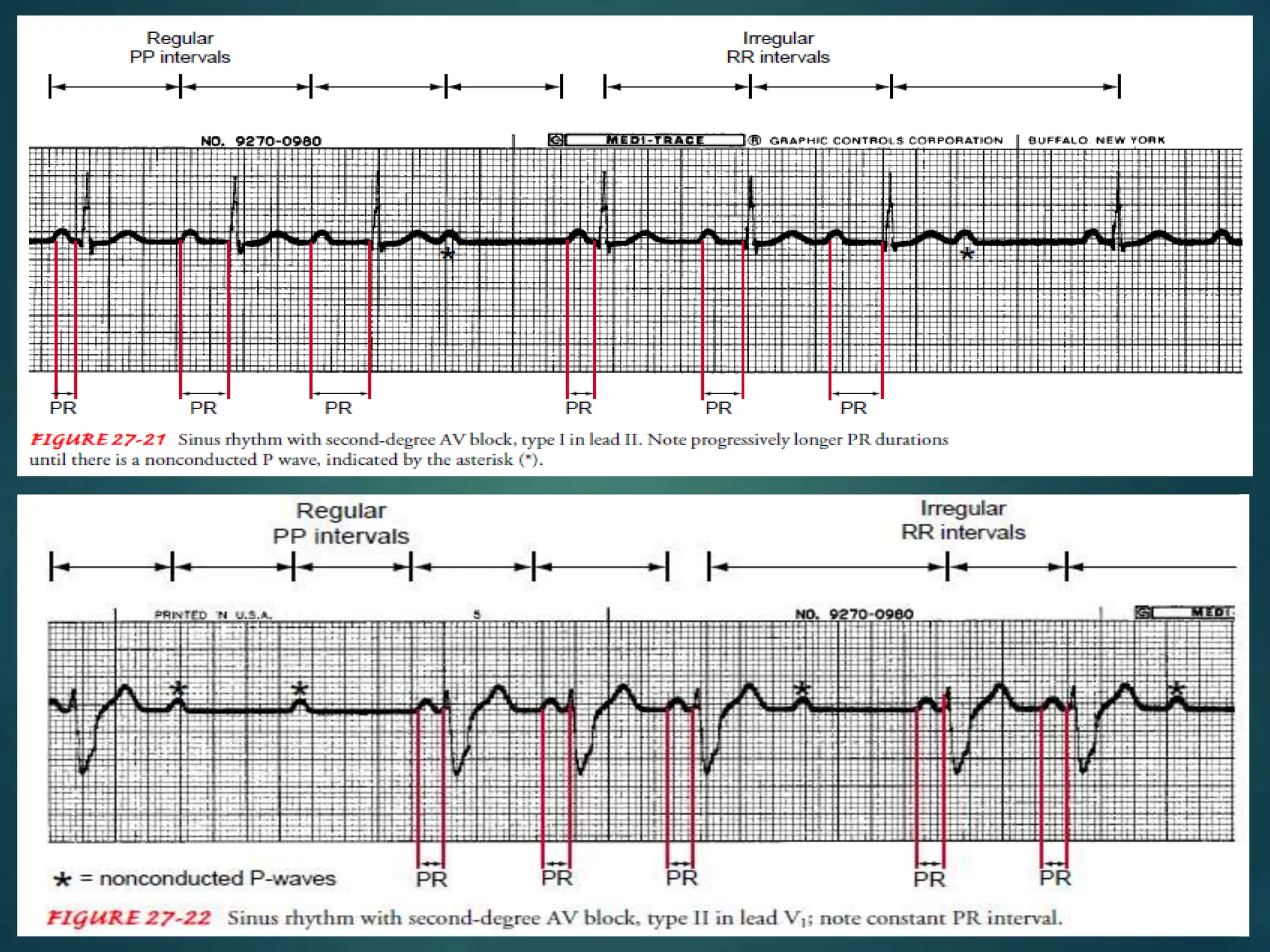
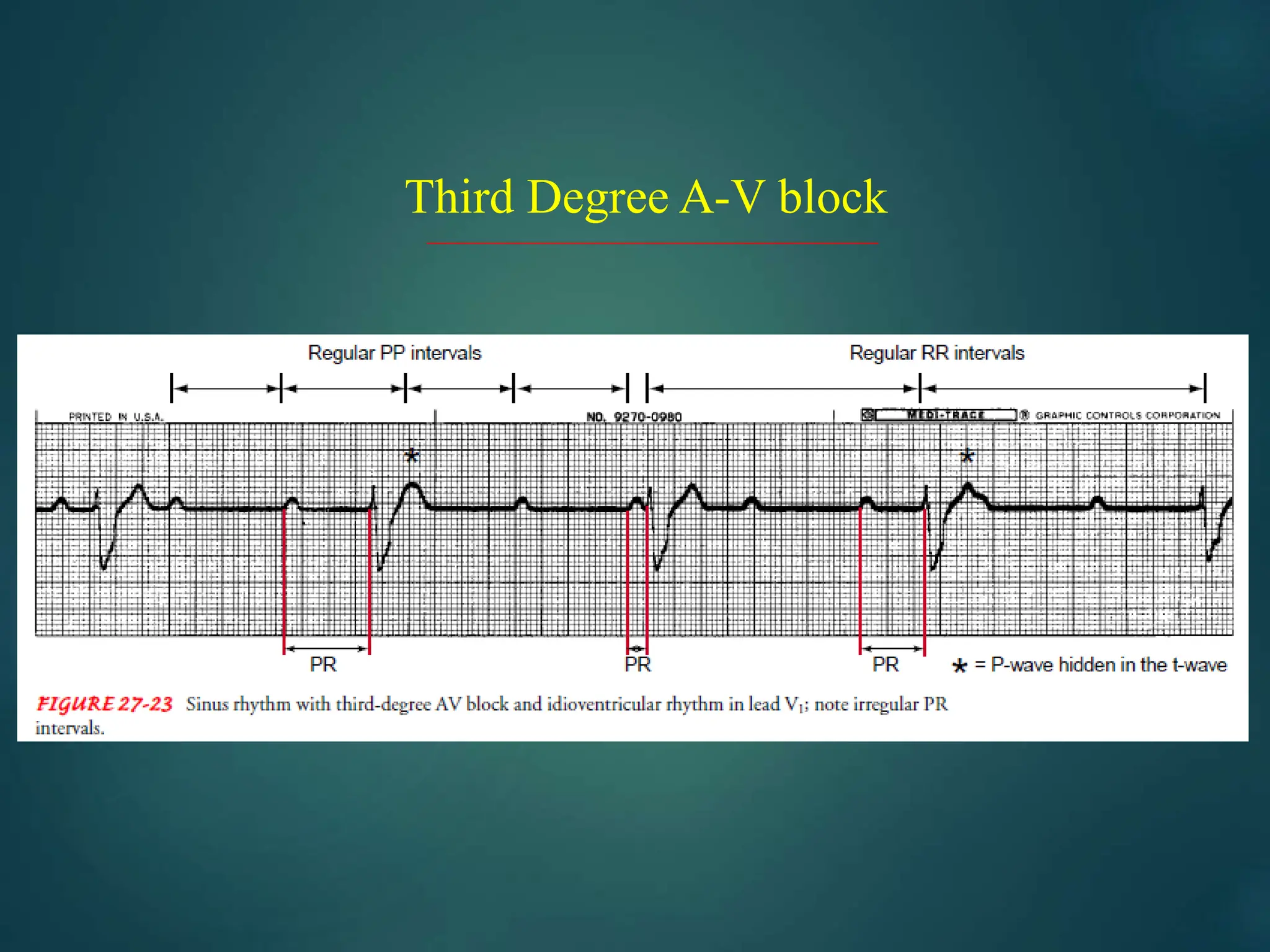
The document discusses various types of atrioventricular (AV) blocks, including first degree, second degree (Mobitz type I and II), and third degree, outlining their clinical significance, ECG characteristics, and management strategies. It highlights that first degree AV block is often benign, while second degree can vary in severity depending on the type, with Mobitz II requiring pacing. Additionally, third degree AV block often necessitates permanent pacing and is commonly seen in the elderly due to various underlying conditions.





















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




